ABIM IM Board Review Pulmonary Physiology and Pulmonary

ABIM IM Board Review Pulmonary Physiology and Pulmonary Function Testing Adam G. Cole, MD Division of Pulmonary, Critical Care and Sleep Medicine

• ~ 8 -12 questions where pulmonary physiology knowledge is needed

Pulmonary Function Testing – Clinical Utility • Define airflow obstruction • Clues to many other pathologic states – Restrictive diseases – Diffusion impairments
")
Spirometry • How much gas can you forcefully exhale? – Forced Vital Capacity (FVC) • How quickly can you blow most of it out? – Forced Expiratory Volume in 1 second (FEV 1)

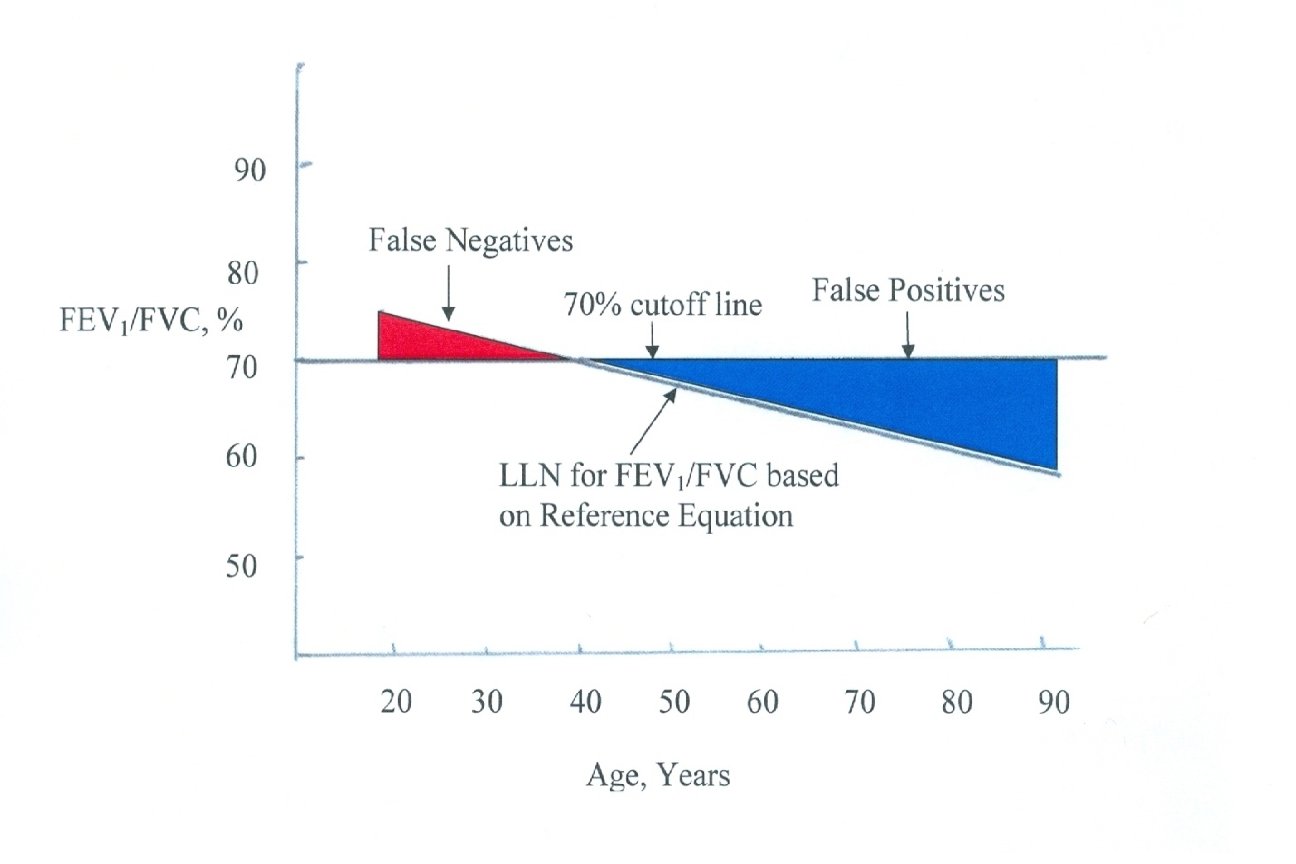
If you remember one thing…. . FEV 1/FVC ratio <70% = Airflow obstruction
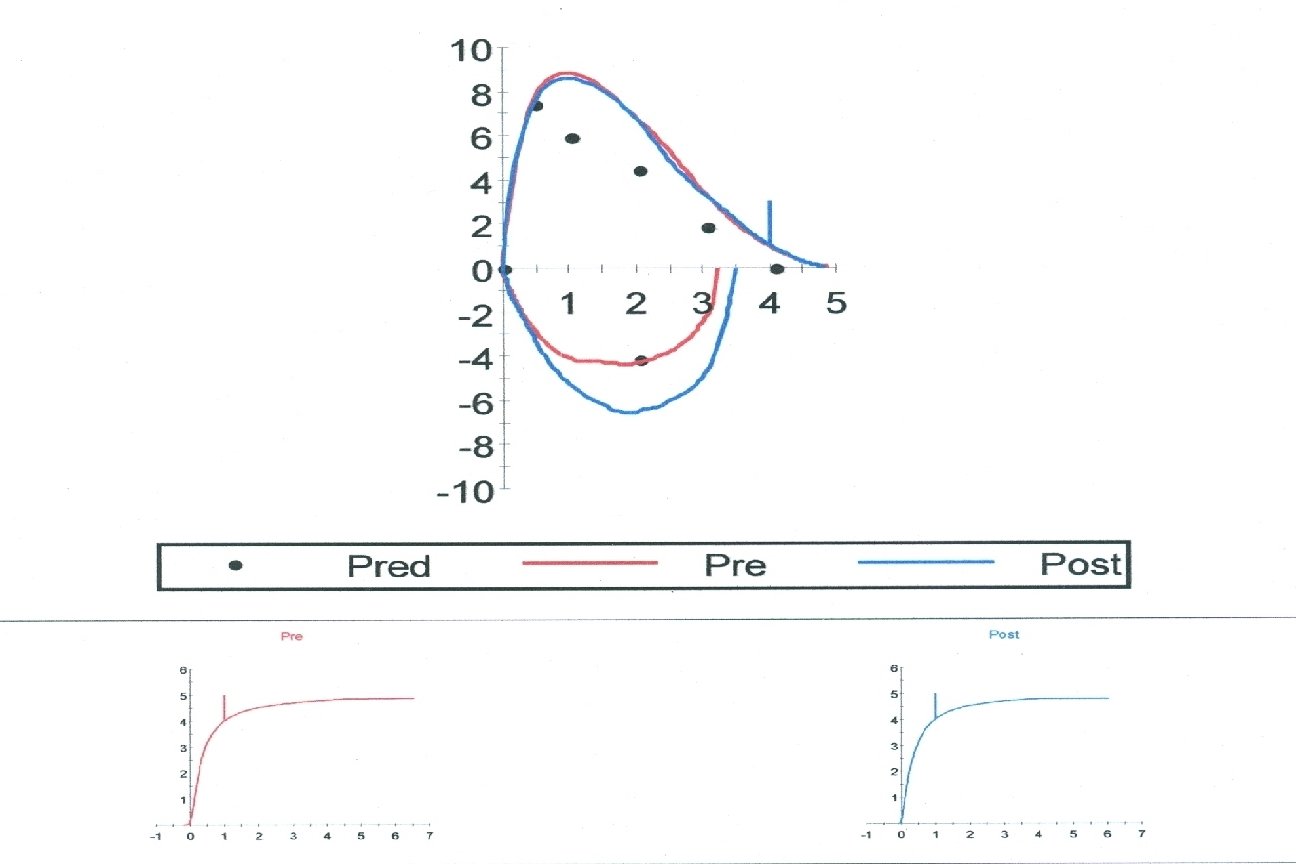

22 yo. F cc severe dyspnea and wheezing. Spirometry shows FEV 1/FVC ratio of 0. 8, FEV 1 of 95% predicted and FVC of 101% predicted. There is no significant response to bronchodilator. Previous methacholine challenge testing was negative. Her flow volume loop is shown in the red (normal on right for comparison): ATS/ERS Task Force: Standardisation of spirometry. Eur Respir J. 2005

What is the next best step in management? A. Start inhaled corticosteroid B. Prescribe albuterol as needed C. Referral for laryngoscopy D. HRCT chest

www. uptodate. com

46 yo. M non-smoker p/w inc’d cough, wheezing and mild dyspnea. These symptoms have been worsening, and are exacerbated by cold air and exercise. Spirometry shows a FEV 1/FVC ratio of 0. 81, FEV 1 of 4. 11 L (95% predicted) and FVC of 5. 05 L (92% predicted). Post bronchodilator spirometry shows FEV 1/FVC ratio of 0. 81, FEV 1 of 4. 25 L (99%) and FVC of 5. 22 L (95%). What is the next best step in management?

What is the next best step in management? A. Obtain methacholine challenge test B. Start Inhaled corticosteroid C. Start albuterol prn D. HRCT chest E. Prednisone burst

Bronchodilator Challenge ≥ 12% ↑ FEV 1 or FVC AND ≥ 200 m. L ↑ |FEV 1| or FVC

Methacholine Challenge • Useful for evaluation for asthma in the setting of normal spirometry without response to bronchodilator • Positive test consistent w/ asthma • Negative test rules it out • Positive test: FEV 1 ↓ ≥ 20% with challenge

67 yo. M cc DOE progressive over the past several years and now he can only walk short distances on flat ground. He has a dry cough, denies chest pain and wheezing. PE: bibasilar velcro rales, mild clubbing. Spirometry shows FEV 1/FVC ratio of 0. 75, FEV 1 of 1. 75 L (62% predicted) and FVC of 2. 5 L (65% predicted). Plethysmography shows a Total Lung Capacity of 62% predicted. What is the most appropriate next test?
 B.")
What is the most appropriate next test? A. Bronchoscopy with BAL (bronchoalveolar lavage) B. Right heart catheterization C. HRCT chest D. Methacholine challenge test
 • Nitrogen washout • Helium dilution •")
Lung Volumes • Body Plethysmography (Body Box) • Nitrogen washout • Helium dilution • Radiographic
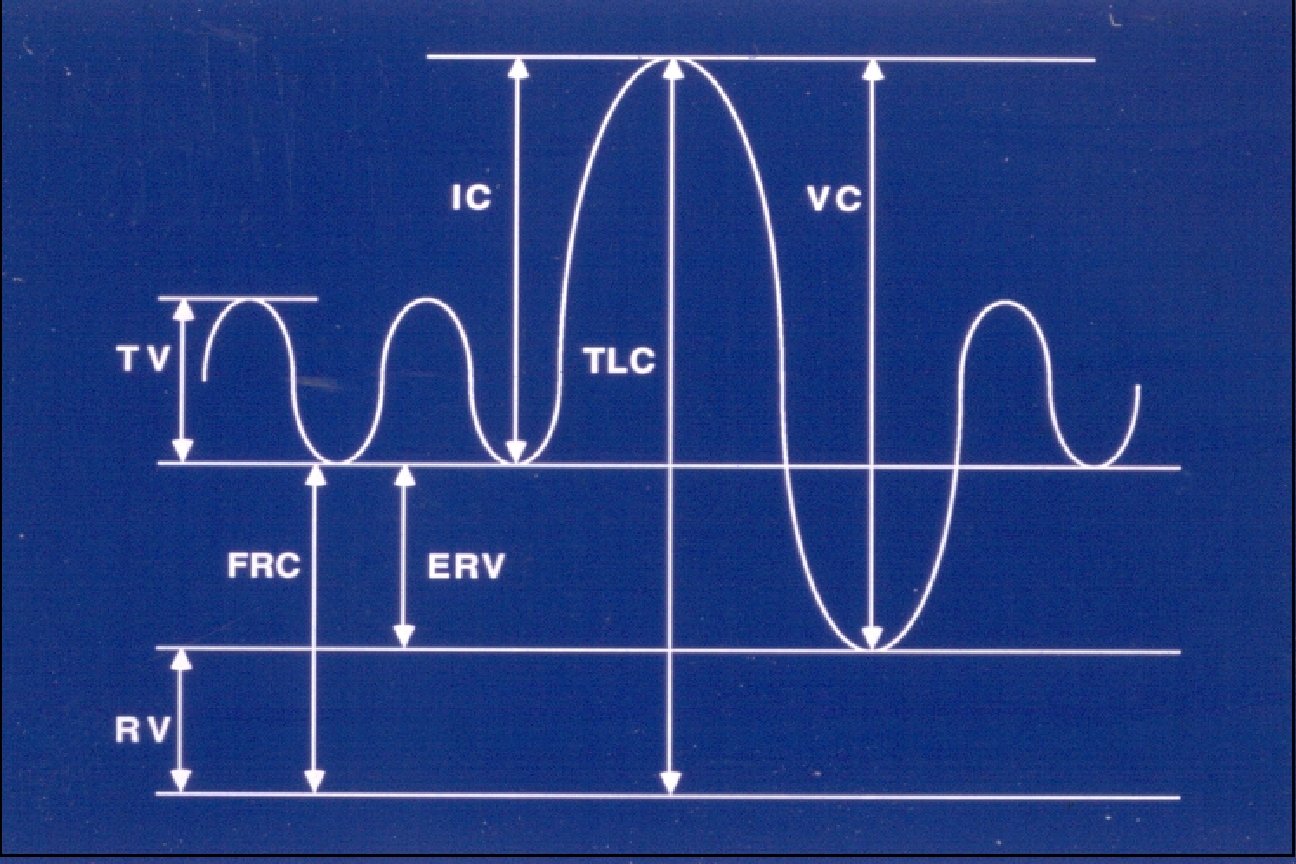

The Numbers…. • TLC < 80% = Restrictive defect • TLC >120% = Hyperinflation • RV > 120% = Air Trapping

Clinical Correlation • TLC < 80% = Restrictive defect • • • Fibrotic ILDs NRO-MSK dz (ALS) Pleural disease Chest wall disorders Obesity

Clinical Correlation • TLC >120% = Hyperinflation – Obstructive diseases • RV > 120% = Air Trapping – Obstructive diseases

36 yo. F cc DOE progressively worsening over 2 years. She was previously active and liked to run, but now she can only walk short distances on flat ground. She denies any cough or wheezing or chest pain. She occasionally feels lightheaded with exertion. HRCT of the chest shows unremarkable lung parenchyma. Spirometry shows FEV 1/FVC ratio of 0. 86, FEV 1 3. 13 L (98% predicted) and FVC 3. 66 L (99% predicted). Plethysmography shows a TLC of 104% predicted. Diffusing capacity (corrected for Hb) is 56% predicted. What is the next best step in management?

What is the next best step in management? A. Methacholine challenge B. Bronchoscopy with transbronchial lung biopsy C. Transthoracic echocardiogram D. Empiric trial of bronchodilators

Diffusing Capacity • Measures ability of lung to take up oxygen

Diffusing Capacity – What to know… • DLCO < 80% predicted = low • Usually corrected for Hb in questions because anemia reduces DLCO

Clinical Correlation • Reasons for low corrected DLCO: –Emphysema –Fibrotic ILDs –Pulmonary vascular disease » Pulm HTN
- Slides: 26