Abdominal wall hernia Hernia strap 1758 What is

Abdominal wall hernia Hernia strap, 1758

What is a Hernia ? Abnormal protrusion of an intra abdominal contents through a defect in the abdominal wall Exception from this definition the epigastric hernia which is a retroperitoneal fat protrusion through a defect in the linea alba

Why Do Hernias Occur? “ETIOLOGY” I. Congenital developmental defect a. Failure of fascial opening to close (e. g. , umbilical) ( if there is a defect in the umbilicus of the infant , usually by time it heals by fibrous tissue. . Sometimes the granuloma of the cut umbilical cord get infected and the collagen become very weak so any increase in the intra abdominal pressure may cause hernia ). b. Failure of process to obliterate e. g. processus vaginalis) in the indirect inguinal hernia collagen metabolism , genetic defects of the c fiber and collagen synthesis, .

II. There is an acquired weakness a. Fascial thinning , Loss of tissue strength and elasticity (from aging or repetitive stress) b. Loss of tissue (injury, infection, poor wound healing, etc. ) c. prolonged or sever increased abdominal (heavy lifting, COPD, )pressure: BPH, ascites Organomegaly , multiple pregnancy , ovarian tumor

Composition of a hernia it consists of three parts: 1. The contents 2. The sac ( peritonium ) In the epigastric hernia there is no sac

3. The covering Umbilical >> skin Para umbilical >> skin Inguinal >> external oblique , internal oblique , skin

Classifications of hernia 1. Anatomical classification: * Groin hernia: inguinal, femoral * Ventral hernia: Umbilical, paraumbilical, epigastric, incisional * Posterior wall hernia : lumber hernia * Pelvic hernia : sciatic hernia , obturator hernia 2. Clinical classification * simple hernia * complicated hernia: - obstructed, - strangulated

Pathological variants of hernia * Incarcerated hernia irreducible , very narrow ring without obstruction of the lumen nor interference with the blood supply * Obstructed * Strangulated hernia If the obstruction is not relived , the edema will interfere with the venous system , increasing the pressure on the arterial system causing strangulation

* Inflamed hernia ( common in dm patients with long standing hernia especially if the content is colon ) Clinically : redness and ulceration in the skin with or without obstruction of the content lumen One of the late sign of strangulated hernia “ changing in the color of the skin “ * Sliding hernia Common if the content : 1 - sigmoid colon 2 - cecum “ part of them is retro peritonium and the other is intra peritonium So it slides and Enter the into the opening , so the sac is not completely covering the organ Common in old age and in the left side of the colon

* Epigastric hernia “ pathological term rather than anatomical term ( no sac , no omentum , no bowel ) ” * Richter’s hernia Part of the circumference or the anti mesenteric border of the bowel is entrapped into the lumen get gangrenous and rated Difficult to diagnosed Normal bowel motion No vomiting … only pain

• Littre’s hernia - In case where the mackle's diverticulum is part of the contents of the inguinal hernia - Very rare known as a hernia in “W” : maydl hernia “ double loops >> more liable to strangulation

Richter’s hernia Littre’s hernia spigelian hernia maydl hernia

Spigelian hernia • Also called interparietal hernia • No posterior rectus sheath at the lower 2/3 of the lower half of the abdomen • At the spigelian fascia ( the curvature at the outer side of the rectus muscle ) with the end of the posterior rectus sheath ( arcuate line )

Clinical features of hernia symptoms 1. A lump a. comes and goes b. appears on standing/straining & disappears when reclining c. size usually increase by time 2. Pain a. dragging in nature b. appears on exertion 3. associated symptoms : nausia, sweating 4. Features of hernia complication d constant pain , Vomiting , constipation abdominal distension

On examining a hernia : The signs - Presence of swelling - the side : left or right - Site of swelling : inguinal, iscrotal, nguinoscrotal - size of swelling - Shape : - skin colour, - scar - Positive visible expansile cough impulse On palpation : - presence of tenderness - skin temp. - Positive palpable cough impulse
")
Sometimes , patient with grid iron incision may have right inguinal hernia ( direct) ? Hernia at site away from the site of the scar ? ? Because during appendectomy the surgeon might injure the ilio-inguinal nerve ( motor to the conjoint tendon and the posterior wall of the inguinal causing weakness and hernia

The signs in strangulated hernia 1. Absence of cough impulse 2. change colour of skin 3. non reducible 4. Tense 5. Tender

Reducibility Depend on the type of hernia : Umbilical + para + direct inguinal > backward Indirect inguinal hernia > upward , laterally then backward Once the hernia is reducible this is a simple hernia

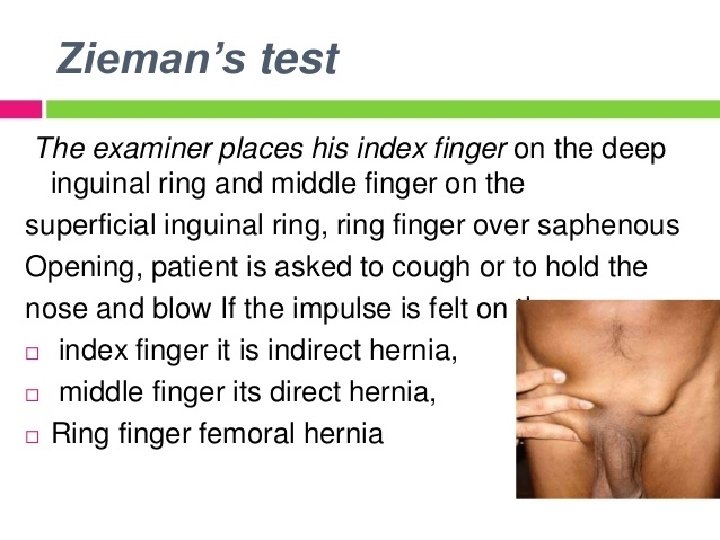
Occlusive test The examiner place his index on the deep inguinal ring , the patient is asked to cough if the impulse is felt this is a direct inguinal hernia

Invagination test Its best used when the hernia is still intra canalicular , , We try to feel the palpable cough impulse while we are in side the canal , , using the little finger

You Cannot go Above the swelling Hernia The swelling is not hernia. . I can feel the content of the cord I cant feel the cord because of the presence of the omentum or bowel


Inguinal Hernia Protrusion through the deep inguinal ring

Indirect inguinal Hernia 1. inguinal hernias representing the most common type of ernia ect inguinal hernias are the most common hernias in both men and women in the groin. In about 10 percent they occur on both sides. 3. it is more frequently on the right side as a result of later descent of the right testis and delayed obliteration of the processus vaginalis. 4. An indirect hernia occurs when a hernia sac enters the deep inguinal ring lateral to the inferior epigastric artery and passes to the superficial ring through the inguinal canal.

Surgical anatomy of the inguinal canal

• The deep inguinal ring >> opening in the transversalis fascia >> 12 ich above the mid point of the inguinal ligament • The superficial inguinal ring >> opening in the external oblique aponeurosis >> ½ ich above the pubic tubercle • The upper half of the inguinal cord anteriorly covered by ( internal oblique and the external oblique aponeurosis • The arching fiber of the internal oblique muscle become the conjoint tendon at the lower half of the cord , so the lower half covered anteriorly by the external oblique aponeurosis

Surgical physiology of inguinal canal The integrity of inguinal canal is maintained by three different shutter mechanisms: er shutter done by contraction of muscle which lift the transversalis fascia sling craniolaterally closing inguinal ring. the deep raction of the internal oblique muscle cover the deep inguinal ring. ontraction of the transversus abdominis arch mes close to inguinal ligament protecting the posterior wall of the canal.

Importance of internal oblique in the shutter mechanism 1 - close the deep inguinal ring by lifting the medial and lateral leafs of the transversalis fascia 2 - pressing on the deep inguinal ring by its contraction 3 - coming near to the inguinal ligament closing completely the posterior wall of the inguinal canal

Types of indirect inguinal hernia 1. Bubonocele 2. Funicular 3. complete

Direct Inguinal Hernia A direct hernia occurs when a hernial sac is pushed through the floor of the inguinal canal medial to the inferior epigastric vessels in Hasselbach Triangle Direct hernias is acquired tend to occur in older patients These hernias rarely move into the scrotum like the indirect inguinal ones. Globular shape rather than funicular

Differential diagnosis 1. Encysted hydrocele of the cord Not reducible , , no cough impulse 2. Spermatocele 3. Femoral hernia etely decended testicle in the inguinal canal 5. Lipoma of the cord 6. Inguinal lymphadenopathy

Femoral Hernia

Femoral Hernia 1. occur about 10 times more commonly in females than they do in males. ne to develop strangulation as an early complication than inguinal hernias. rnia the hernia sac is pushed into the oral canal, below the inguinal ligament and between the lacunar ligament and the femoral vein. the hernia sac thus lies inferior and lateral to the pubic tubercle

Protrusion from the most medial compartment of the femoral canal between the femoral sheath and the lacunar ligament

Differential diagnosis 1. Inguinal hernia 2. Saphena varix (big long dilated saphenous vein >> true compressible test ) 3. Enlarged femoral lymph node 4. Lipoma 5. A femoral aneurysm 6. Psoas abscess ( in pott TB )

Incisional Hernia

Incisional Hernia 1. most common type of ventral hernia otrusion of viscos through a defect in a previous surgical incision 3. and occurs in 5 – 10 % of abdominal incision uses behind are related to patient factors and operation factors ent within 12 months postarotomy although as many as 1/3 may present 5 -10 years later eatment primary suture repair or prosthetic mesh repair

What are the risk factors for developing an incisional hernia? 1. Patient-related factors: a- malnutrition, diabetes mellitus, corticosteroids, Hypoprotinemia , vit c deficiency , ca and mg deficiency ( wound healing related factors ) b- conditions that increase intra-abdominal pressure like ascites, chronic cough, urinary outflow obstruction 2. Surgery-related factors: a- wound infection, b- closure of abdomen under tension, c- type and location of incision (vertical midline incision more prone to incisional hernia than transverse), also incision in the lower abdomen more liable for hernia then that in the upper

Umbilical Hernia

Umbilical Hernia 1. It may be congenital or acquired mbilical hernias are most common in infants, but they can affect adults as well. The umbilical hernia occurs through the umbilical fibromuscular ring, which usually obliterates by ars of age and are repaired if they persist in children older than age 2 -4 ers had several pregnancies are prone to umbilical hernias

Hernia management in general 1. The complicated hernia “strangulated” : Needs Ergent Operation a. resuscitation of the patient eleive the obstruction, if not gangrenous reduce the content back. c. repair of the defect

2. Elective hernia management Pre operative: The precipitating factors should be managed Operative. Treatment a. Herniotomy. Herniorrhaphy is achieved by closing the defect in the strong layer of the abdominal wall c. hernioplasty c material called a “mesh” is nly utilized in repairing the defect in order to add extra strength. Post opoerative care: avoidance factors lead to hernial recurence

Hernia Repair Complications 1. Wound: - Hematoma: 1 -2 days after operation - Infection: 3 days after operation - Seroma : 1 -2 days after operation 2. Vascular injury - Ischemic orchitis is uncommon 3. Nerve injury: 4. Visceral injury - Injury to vas deferens - bowel -urinary bladder ( in direct hernia )

3 nerves and vessels liable to injury during hernial correction surgery Nerves : 1 -iliohypogastric 2 - ilioinguinal 3 - genital branch of the genitofemoral nerve Vessels : 1 - inferior hypogastric 2 - testicular artery 3 -
- Slides: 46