Abdominal Tuberculosis Lymphadenopathy TB Peritonitis Introducton Most common

Abdominal Tuberculosis Lymphadenopathy TB Peritonitis

Introductıon Most common extrapulmonary TB Abdominal LAP: most common manifestation Solid viscera affected more than GI 55%-66% of patients TB peritonitis: most common clinical manifestation Wet Fibrotic Dry frequency CT is best; consider other modalities to avoid misdiagnosis e. g. Barium Enema Primarily hematogenous spread but also 2 y to: • Ruptured LN • GI deposit • Fallopian tube inv.
 have: Enlarged nodes")
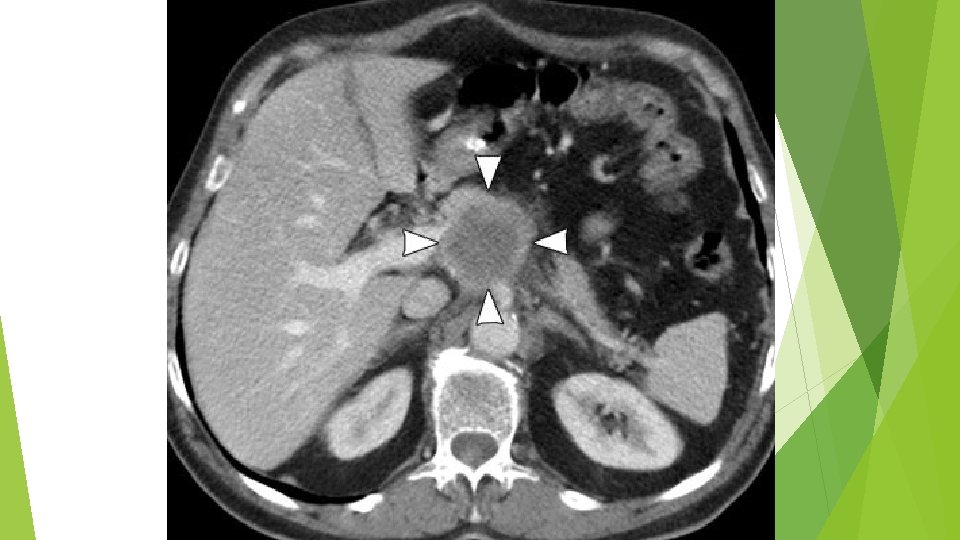
CT Evaluation: LAP Mesenteric and peripancreatic LN group enlargement Majority (40%-60%) have: Enlarged nodes w/ hypodense centers and hyperdense rims Characteristic, but not pathognomic, for caseous necrosis LAPs usually don’t cause obstructive symptoms (Biliary, GI, GU) via mass effect If present, consider other pathology
")
CT Evaluation: wet peritonitis Large amounts of free or loculated ascites (20 -45 HU) High cellular and protein content

CT Evaluation: fibrotic peritonitis Characterized by: large omental and mesenteric cakelike masses with matting of bowel loops Manifests as mottled hypodense masses with nodular soft-tissue thickening Omental caking and thickening detectable via USG

CT Evaluation: dry peritonitis Characterized by: mesenteric thickening, fibrous adhesions, and caseous nodules Imaging manifestations (↑ suggestive but non-specific for TB): Omentum Smudged, caked, or thickened Mesentery Involvement ranges from mild to extensive Peritoneum Thickening with associated enhancement Nodular implants with irregular thickening uncommon; think peritoneal carcinoma
- Slides: 7