Abdominal Trauma Begashaw M MD Anatomy Abdominal Trauma
")
Abdominal Trauma Begashaw M (MD)

Anatomy

Abdominal Trauma Ø Two mechanisms _Blunt usually causes solid organ injury (spleen injury is most common) _Penetrating usually causes hollow organ injury or liver injury (most common)

Mechanism of Injury l Blunt Force Trauma l Penetrating Trauma

Mechanism of Injury Africa style

Mechanism of Injury l Blunt – Speed – Nature of Impact – Position in vehicle – Ejection – Intrusion – Seatbelt – Airbag l Penetrating – Type of weapon – Distance – Number and location of wounds – Trajectory – Energy – Blast effect

BLUNT TRAUMA l results in two types of hemorrhage - intra-abdominal bleeding - retroperitoneal bleeding l adopt high clinical suspicion of bleeding in multi-system trauma

Examination Abdomen Inspect: contusions, abrasions, seatbelt sign, distention Auscultate: bruits, bowel sounds Palpate: tenderness, rebound tenderness, rigidity, guarding DRE: rectal tone, blood, bone fragments, prostate location Placement - NG, foley catheter Ø

Commonly injured organs l Spleen l Liver l Small Bowel
 _Altered")
Assessment of abdominal trauma l Difficult due to: _Altered sensorium (head injury, alcohol) _Altered sensation (spinal cord injury) _Injury to adjacent structures (pelvis, chest)

Investigations l Labs: CBC, electrolytes, cross & type, glucose, creatinine, amylase, liver enzymes l Imaging

Imaging strengths limitations X-ray Erect CXR Soft tissue not visualized CT scan Most specific test Radiation, cannot use if hemodynamic instability Diagnostic peritoneal Lavage Most sensitive test Test for intra abdominal bleeding Retroperitoneal hemorrhage, diaphragmatic rupture Ultrasound FAST Free fluid, Rapid, pericardium, plura Specific organ injury

FAST Focused assessment for the sonographic assessment of trauma Ø Assess for intraperitoneal fluid o Right upper quadrant o Left upper quadrant o Suprapubic region Ø Fluid in subphrenic, subhepatic spaces or Pouch of Douglas in hypotensive patient l Confirms likely need for emergency laparotomy l

FAST

Criteria for positive DPL l >10 cc gross blood l Bile, bacteria. foreign material l RBC count >I 00, 000 l WBC >500 l Amylase > 1751 U

Imaging l Equivocal abdominal examination, suspected intra-abdominal injury l Multiple trauma l Unexplained shock/hypotension l Fractures of lower ribs, pelvis, spine l positive FAST

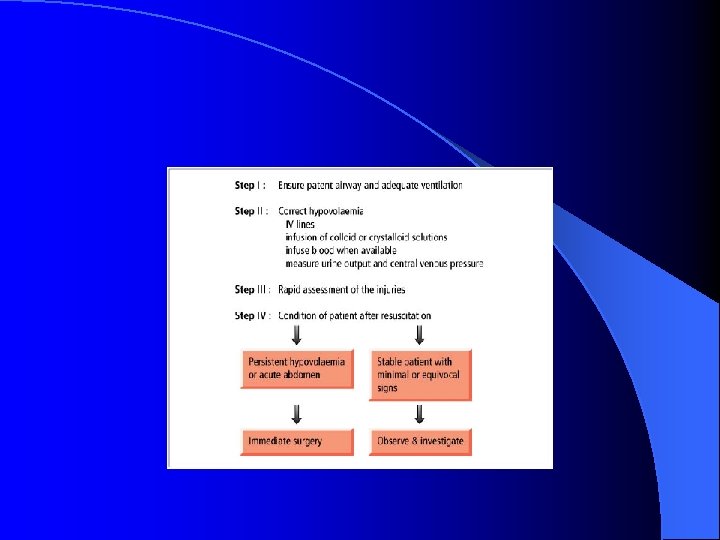
Management l l l General: ABCs, fluid resuscitation and stabilization Surgical: watchful wait vs laparotomy Solid organ injuries: decision based on hemodynamic stability, not the specific injuries Hemodynamically unstable or persistently high transfusion requirements: laparotomy Hollow organ injuries: laparotomy Even if low suspicion on injury: admit and observe for 24 hours

Indications for Laparotomy l Free Fluid on FAST l Unstable patient with suspected abdominal injury l Free Air l Diaphragm Rupture l Peritonitis l Positive findings on CT Scan

PENETRATING TRAUMA High risk of gastrointestinal perforation and sepsis History: size of blade, calibre/distance from gun, route of entry l Local wound exploration under direct vision may determine lack of peritoneal penetration (not reliable in inexperienced hands) with the following exceptions: -thoracoabdominal region (may cause pneumothorax) -back or flanks (muscles too thick) l l

Penetrating Trauma l Overall condition of the patient l Local wound exploration l DPL?

Penetrating abdominal trauma

Laparomy in penetrating injury l Shock l Peitonitis l Eviseration l Free air in abdomen l Blood in NG tube, Foley catheter, or on rectal exam

Management Ø General: ABCs, fluid resuscitation and stabilization l Gunshot wounds-always require laparotomy
- Slides: 24