Abdominal injury and Management Dr Mohammadzadeh 13 Feb

Abdominal injury and Management Dr. Mohammadzadeh 13 Feb 2013

Background • Traumatic injury is the leading cause of morbidity and mortality in children >1 year in U. S. • Trauma to the abdomen is often initially unrecognized • Abdominal trauma accounts for 8 -10% of all trauma admissions to peds hospitals • Blunt injuries account for > 80% admits ATLS, 7 th Edition, 2004

Factors Unique to Pediatrics • Anatomic – Larger relative size of solid organs – Rib cage and abdominal muscles less protective – Bladder intraabdominal until adolescence – Large head: often have multisystem injury • Physiologic – Hypotension is a late finding in shock – Increased relative surface area prone to hypothermia ATLS, 7 th Edition, 2004

Mechanism • Blunt abdominal trauma • Penetrating abdominal trauma • Overall about 20% require surgical operation
 injury • Seat belt injury")
Blunt abdominal trauma • Motor vehicle crush ( MVC) injury • Seat belt injury • Handle bar injury • Fell from height

Penetrating abdominal injury • • Stab wound – low energy transfer Gun shot wound – high energy transfer

Anatomy • Between diaphragm and pelvic floor • Beware of diaphragmatic injury in penetrating chest injury below the nipples (5 th ICS) • Mid-axillary line • Retro-peritoneal spaces – zone I, II & III

anatomy Ø Anterior abdomen Ø flank Ø Back Ø intraperitoneal contents Ø Retroperitoneal space contents Ø Pelvic cavity contents

o Anterior abdomen: trans-nipple line, , anterior axillary lines, inguinal ligaments and symphysis pubis. o flank: anterior and posterior axillary line ; sixth intercostal to iliac crest o Back: posterior axillary line; tip of scapula to iliac crest

• Peritoneal cavity: upper-diaphragm, liver, spleen, stomach, and transverse colon; lowersmall bowel, sigmoid colon • Retroperitoneal space: aorta, inferior vena cava, duodenum, pancreas, kidneys, ureters, ascending and descending colons • Pelvic cavity: rectum, bladder, iliac vessels and internal genitalia
 • Hollow organs – blood,")
Anatomy • Solid organs – liver, spleen, kidney (blood) • Hollow organs – blood, bile, urine, food, digestive juice, air • Remember the diaphragm which is neither solid nor hollow organ

First step of Management • Resuscitation of patients with suspected abdominal injuries – same as other trauma patients • ATLS • Surgical plan
 • Is")
Basic plan of Surgical Decision • Is there any abdominal injury? (PE) • Is intervention required? (conservative treatment + close monitoring +/- serial Ix) • Is surgery required? (interventional radiology) • Damage control or definitive surgery (correct physiology then anatomy)

Assessment and diagnosis • Normal abdominal finding • Obvious injury to the abdomen eg gun shot wound • Equivocal findings requiring further investigation and re-assessment eg blunt abdominal trauma
")
Investigations • • Diagnostic peritoneal lavage DPL FAST USG CT scan (Laparoscopy)

DPL • • • Previously the standard investigation Replaced FAST Detect blood Bowel content : bacteria, food particles, bile Accuracy up to 98% Miss diaphragmatic and retroperitoneal injury

Diagnostic Peritoneal Lavage
 • Amount of warmed Ringer’s lactate for lavage: – 10")
Diagnostic Peritoneal Lavage (DPL) • Amount of warmed Ringer’s lactate for lavage: – 10 ml/kg in a child – 1 liter in an adolescent/adult • Positive DPL: – >100, 000 RBC/mm 3 – >500 WBC/ mm 3 – Gram stain with bacteria – Aspiration of gross blood, GI contents, vegetable fibers, or bile ATLS, 7 th Edition, 2004
 inside peritoneal cavity Accuracy comparable to DPL Non")
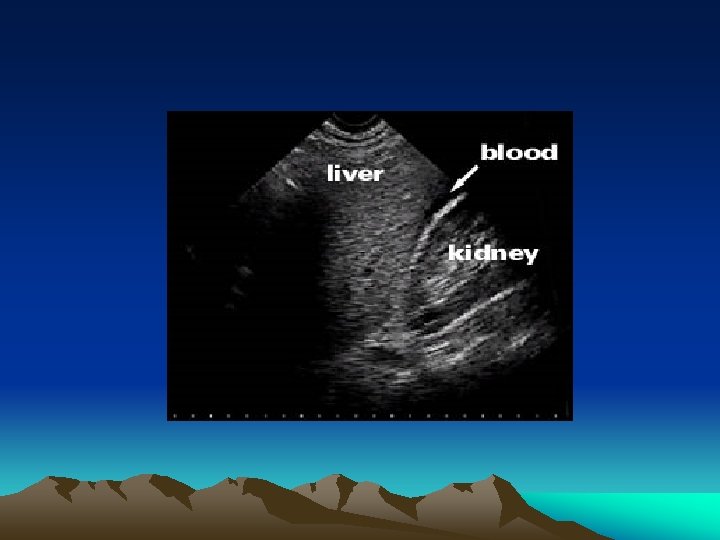
FAST • • Detect fluid (blood) inside peritoneal cavity Accuracy comparable to DPL Non invasive and repeatable Operator dependant Miss specific injuries Obesity Replace DPL in many trauma centre

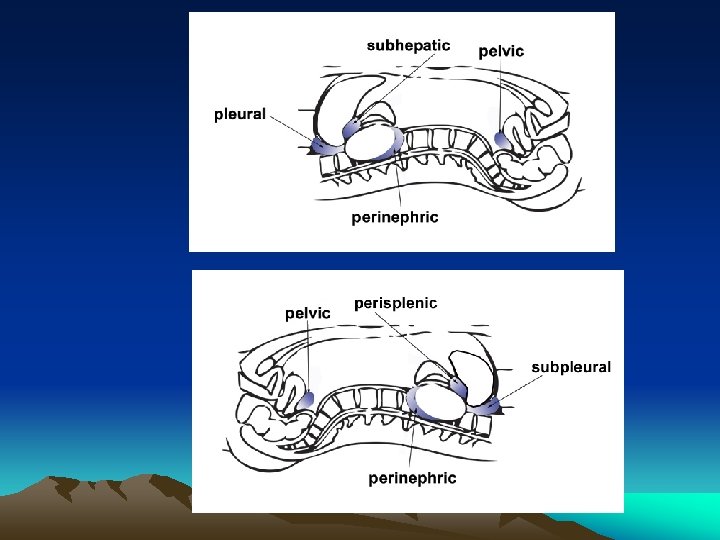
FAST • Focused areas of exam: – Hepatorenal fossa – Splenorenal fossa – Pericardial sac – Pelvis (pouch of Douglas)

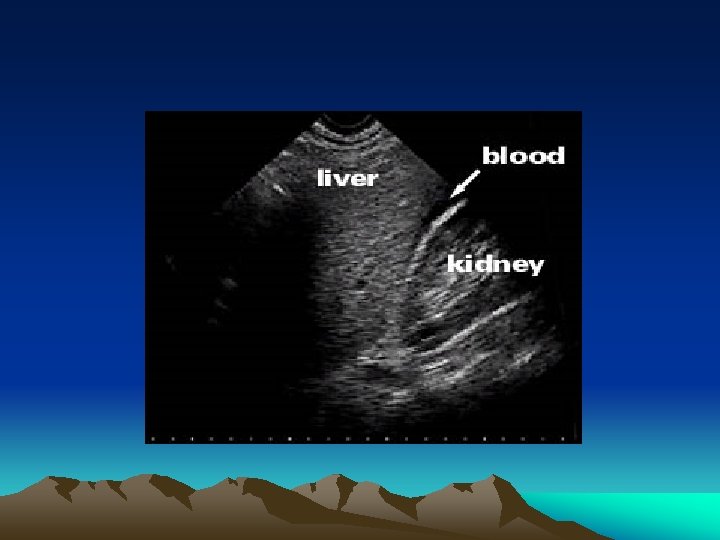
Hepatorenal view normal

Hepatorenal view abnormal

Splenorenal view

FAST in Pediatrics • Multiple studies have prospectively evaluated FAST with CT +/- ex lap as a gold standard • Results are variable: – Sensitivity: 70 -80% – Specificity: 97 -100% Suthers, et al. Am Surg. 2004 Feb; 70(2): 164 -7 Corbett, et al. Am J Emerg Med. 2000 May; 18(3): 244 -9 Thourani, et al. J Pediatr Surg. 1998 Feb; 33(2):

CAT scan • • • Document specific organ injury Retro-peritoneal organs Accurate Haemo-dynamically stable patients Can still miss diaphragmatic injury and bowel injury
 • Lifetime cancer mortality risk attributed to radiation exposure in 1")
Computerized Tomography (CT) • Lifetime cancer mortality risk attributed to radiation exposure in 1 year old: – Abd CT: 0. 18% – Head CT: 0. 07% • 500 out of 600, 000 children will die secondary to malignancy from radiation exposure Brenner, et al. Am J Roentgenol. 2001 Feb; 176(2):
 • Reasons to scan: – Abdominal tenderness with hematuria – Low")
Computerized Tomography (CT) • Reasons to scan: – Abdominal tenderness with hematuria – Low GCS – + FAST in stable pt • Reasons not to scan: – Normal exam Richards, et al. Am J Emer Med. 1998 Jul; 16(4):

Spleen/Liver • Contrast enhanced CT has 95% sensitivity and specificity for diagnosing splenic and hepatic injuries Minarik, et al. Pediatr Surg Int. 2002 Sep; 18(5 -6):

Bowel injury • Less sensitive/specific for hollow viscous injury • Nonspecific findings common • Serial exams most inportant

Pancreas • Of 1045 children with BAT, 18 sustained injuries seen on autopsy, laparotomy, or clinically – 13/18 seen on CT with fluid in lesser sac – SN = 72%; SP = 99% Sivit, et al. Am J Roentgenol. 1992 May; 158(5): 1097
")
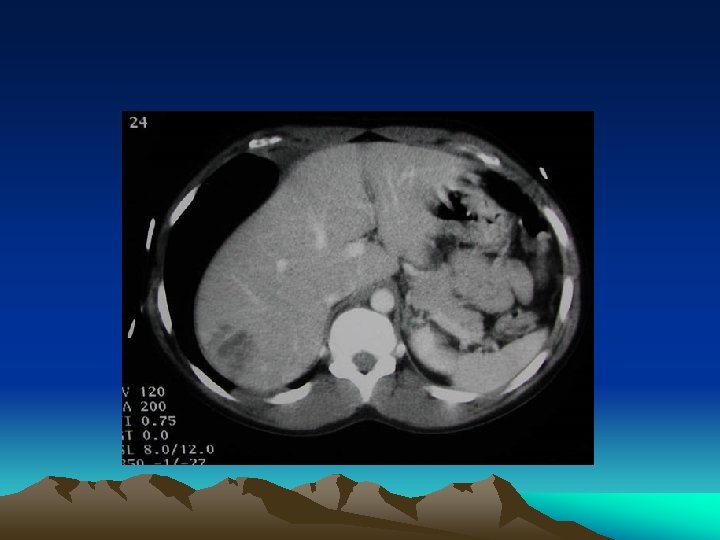
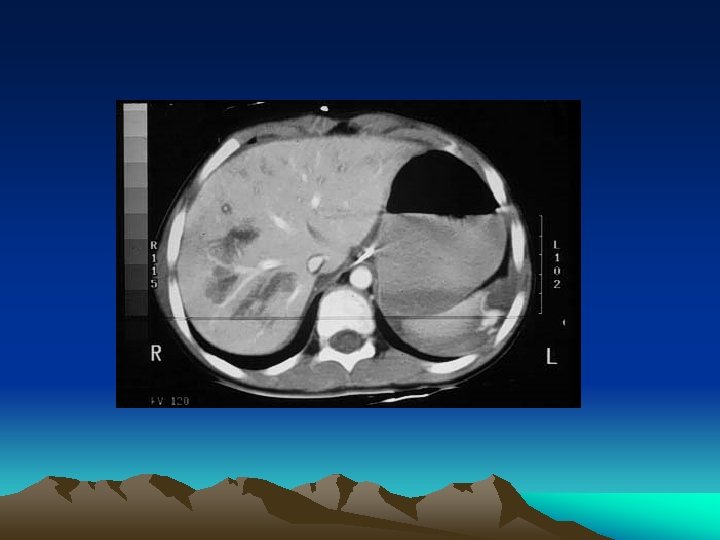
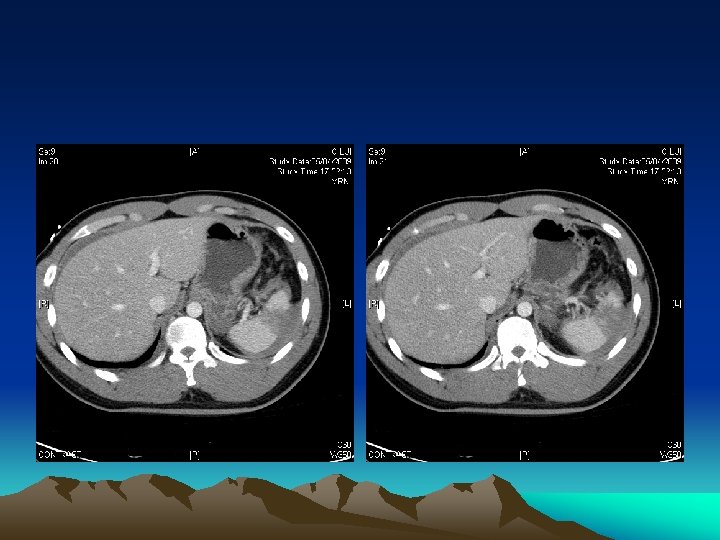
Renal Laceration (Grade IV)
")
Renal Laceration (Grade IV)
")
Renal Laceration (Grade IV)
 •")
Basic plan of Surgical Decision • Is there any abdominal injury? (PE, Ix) • Is intervention required? (conservative treatment + close monitoring +/- serial Ix) • Is surgery required? (interventional radiology) • Damage control or definitive surgery (correct physiology then anatomy)

Surgical decision • Normal abdominal finding • Obvious injury to the abdomen • Equivocal abdominal findings

Normal abdominal finding • Re-assessment and physical finding by same experienced surgeon in haemodynamically normal is usually sufficient • ? CAT scan before other extra-abdominal surgery in awake and alert patients • FAST or DPL in unstable patients

Surgical decision • Normal abdominal finding • Obvious injury to the abdomen • Equivocal abdominal findings





Obvious injury to the abdomen • Mostly applied to penetrating injury • Virtually all penetrating abdominal injury should be “explored” promptly, especially in the presence of hypotension • Local wound exploration • Laparoscopy / laparotomy • Gun shot wound - laparotomy • CAT scan

Surgical decision • Normal abdominal finding • Obvious injury to the abdomen • Equivocal abdominal findings

Equivocal abdominal findings • Further investigation very much depends on haemo-dynamic status of the patients • Haemodynamically normal: reassessment , CAT scan, other investigation


Equivocal abdominal findings • Haemodynamically stable : CAT scan • Whether the patient has bled into the abdomen • Whether the bleeding has stopped. • Detect specific organ injury

Equivocal abdominal findings • What if CT shows free fluid without solid organs injury in a stable patient? • Blood, bowel content, bile, urine • ? Mandatory laparotomy • But non-therapeutic laparotomy is up to 92% in one of the US multi-centre prospective study • Re-assessment

Equivocal abdominal findings • Haemodynamically unstable : DPL or FAST • Positive finding : operation • A negative finding is also important : we have to focus on the other compartment (chest, pelvis, long bones) or external haemorrhage
 •")
Basic plan of Surgical Decision • Is there any abdominal injury? (PE, Ix) • Is intervention required? (conservative treatment + close monitoring +/- serial Ix) • Is surgery required? (interventional radiology) • Damage control or definitive surgery (correct physiology then anatomy)
 • Splenic")
Conservative management • NOM • Liver injury (esp grade I – III) • Splenic injury (esp grade I – III, paediatric group) • Renal injury • Interventional radiologist

Conservative management • Beware of concomitant solid and hollow organ injury • ~7% • It is still safe to adopt non operative management to stable patients with solid organ injury patients but repeated assessment is required
 •")
Basic plan of Surgical Decision • Is there any abdominal injury? (PE, Ix) • Is intervention required? (conservative treatment + close monitoring +/- serial Ix) • Is surgery required? (interventional radiology) • Damage control or definitive surgery (correct physiology then anatomy)

Is urgent surgery required? • • • Radiological evidence of intraperitoneal gas Radiological evidence of ruptured diaphragm Gunshot wounds Evisceration Positive result on diagnostic peritoneal lavage Rigid silent abdomen or unexplained shock

Aim of urgent operation • Haemorrhage control • Contamination control • Anatomical repair



Aim of urgent operation • • Haemorrhage control Contamination control Anatomical repair Haemorrhage control + contamination control – anatomical repair = damage control surgery

Damage control • US Navy, term used for battle ship • staged laparotomy, surgical resuscitation, temporary abbreviated surgical control (TASC) • Focus on restoring function / physiology • Defer treatment of structural / anatomical disruption • Temporary abdominal closure
 • Combined vascular, solid")
Damage Control Surgery • Inability to achieve haemostasis (liver injury) • Combined vascular, solid and hollow organs injury • anticipated need for time consuming procedure • Demand for other control of other injury • Inaccessible major venous injury • Evidence of poor physiological reserve (acidosis, hypothermia, coagulopathy)


Role of laparoscopy • Both as diagnostic and therapeutic tools • Particularly good in detecting diaphragmatic injury • Operator dependant • Difficult to do full trauma evaluation – esp retro-peritoneal space

Role of laparoscopy • Contraindication : haemodynamically unstable patient • Uses in stable patients 1. Stab wound after LWE 2. Fever or raised WBC in patient under NOM, such as in case of liver laceration

Interventional radiologist • Work with arteries • Cannot help in hollow organ injuries except drainage of post op collection • Common sites : liver, spleen, pelvis • Contra-indication : haemodynamically unstable patients (except after damage control procedure in some scenario) • Organ infarction

Interventional radiologist

Specific organs injury

Liver Anatomy

Liver Laceration GRADE DESCRIPTION I < 1 cm parenchymal depth II Depth 1 -3 cm, < 10 cm in length III Depth > 3 cm IV 25 -75% of hepatic lobe V > 75% of hepatic lobe

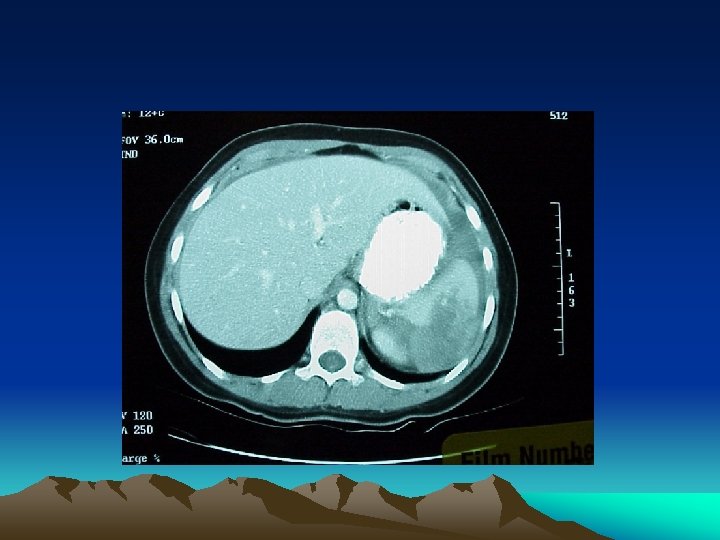
Grade 4 Liver laceration

Hepatic injury • Grade I to VI • VI – hepatic avulsion • Contrast CT scan - very accurate in diagnosis and grading • Conservative treatment : stable low grade injury • Angiographic embolization : higher grade injury with evidence of continuous bleeding • Surgery : Unstable patients

Surgery in hepatic injury • Pringle manoeuvre (occlusion of both inflow to liver ie. portal vein and hepatic arteries. ) • Failed to control bleeding => aberrant Lt or Rt hepatic arteries or retro-hepatic venous injury • Parenchymal suture • Peri-hepatic packing • Consider embolization • Bile leak

Splenic Lacerations GRADE I DESCRIPTION IV Subcapsular hematoma <10% surface area Laceration <1 cm in depth Subcapsular hematoma 10 -50% surface area Laceration 1 -3 cm in depth w/o vessels involved Intraparenchymal hematoma <5 cm diameter Subcapsular hematoma >50% surface area or expanding/ruptured hematoma Laceration >3 cm in depth or w/ vessels involved Intraparenchymal hematoma >5 cm diameter Devascularization of >25% of spleen V Shattered spleen or hilar vascular injury II III

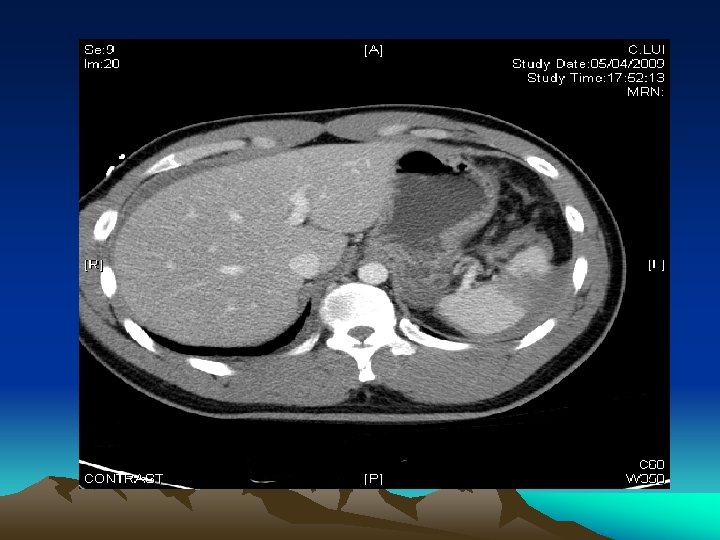
Grade 5 splenic laceration

Grd 4 -5 splenic laceration

Splenic injury • Grade I – V • V – shattered spleen or hilar vascular injury • Conservative treatment (children, stable, intraabdominal injury, no significant brain injury) • Angiographic embolization (even up to 80% in grade IV to V stable patients in one study, Hann JM 2005) • Suturing, wrap, total or partial splenectomy

Pancreatic Anatomy

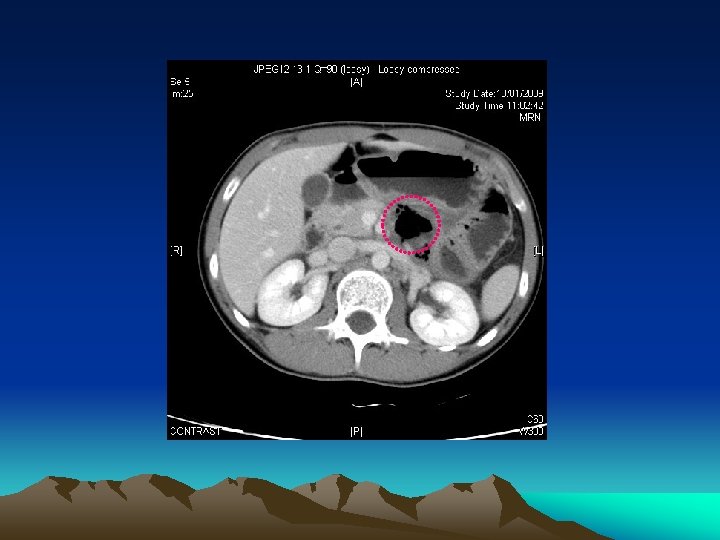
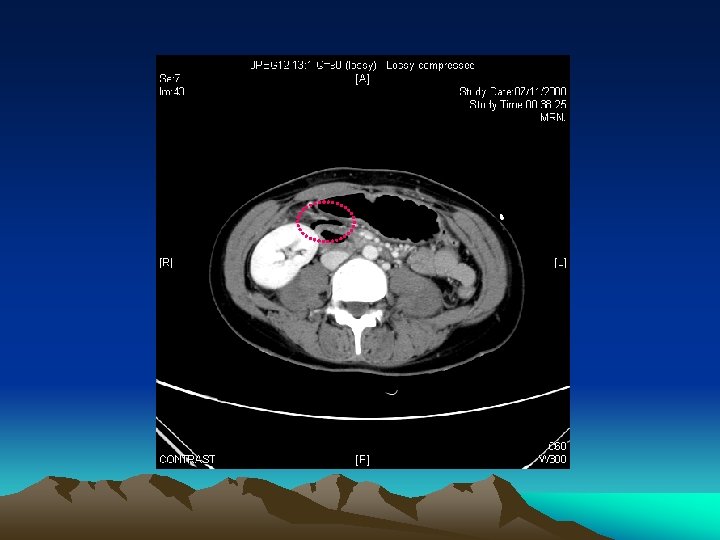
Pancreatic injury • • Grade I – V Grade I & II – intact main duct blunt injury (steering wheel, handle bar) Retro-peritoneal structure => not much peritoneal sign • Amylase level not reliable in initial evaluation • CAT scan (contrast)
 but not sensitive (~50%)")
Pancreatic injury • 1. 2. • CT scan Specific (>90%) but not sensitive (~50%) May require repeated scan ERCP to assess main duct integrity (in EDU or intra-op)

Pancreatic injury • Grade I, II cases => closed suction drainage (in selected cases NOM) • Grade III – V => resection. • Common site of injury at neck which is compressed against the spine => distal pancreatectomy with splenic preservation

Pancreatic injury

Pancreatic injury

Pancreatic injury

Pancreatic injury
 should")
Bowel injury • • Bowel perforation (peritonitis, free gas, bowel content in DPL) should never be treated by non-operative management Small bowel injury – primary anastomosis Colonic injury – colostomy or primary anastomosis +/- second look laparotomy Duodenal injury – retroperitoneal sturcture

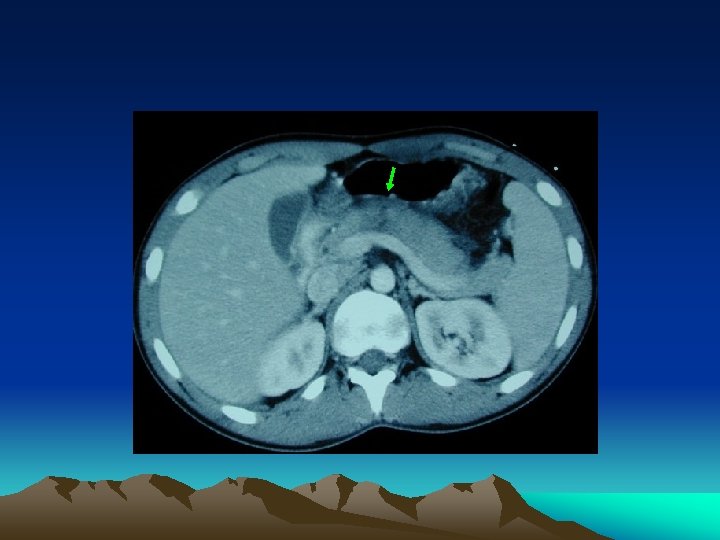
Duodenal injury • Even perforation, abdominal sign not florid • May required extensive mobilization of surrounding structure for repair • Duodenal haematoma after a blunt injury can be managed by conservative treatment

Handlebar Injury

Duodenal Hematoma

Duodenal Hematoma

Renal injury

Kidneys and Urinary Tract
 Hematoma: subcapsular, nonexpanding")
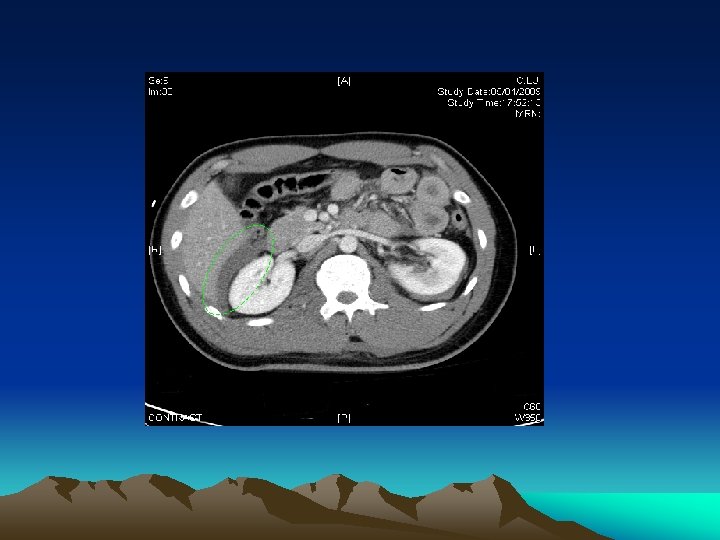
Renal Injury GRADE I II IV V INJURY Contusion: hematuria (micro/gross) Hematoma: subcapsular, nonexpanding w/o parenchyma involved Hematoma: perirenal, nonexpanding Laceration: <1 cm depth Laceration: >1 cm depth Laceration: through cortex, medulla, collecting system Vascular: main artery/vein injured; bleed confined Laceration: completely shattered kidney Vascular: complete hilar avulsion
 Contrast CAT scan")
Renal injury • • • Grade I to V Haematuria (30%) Contrast CAT scan Angiographic embolization Urinoma, sepsis, hypertension

Abdominal compartment syndrome • Sequestration of fluid and edema of bowel wall and mesentery • Increase intra-abdominal pressure => decrease perfusion of viscera => further increase capillary leakage in bowel wall causing a viscous cycle • oliguria, increase peak inspiratory pressure, increase CVP & PAWP (false), decrease cardiac output

Abdominal compartment syndrome • • Indirect measure through Foley catheter Normal < 5 mm. Hg <25 mm. Hg – fluid resuscitation >25 mm. Hg + oliguria with adequate blood volume => consider decompression • Bogota bag, sandwich-vacuum closure, other commercial packs



Thank you
- Slides: 113