Abdominal imaging pathologies and protocols Jason Elliott Session

Abdominal imaging: pathologies and protocols Jason Elliott

Session Structure Radiographer style approach • Justification • Review of standard views – When and why • The “Normal” Abdomen – Structures and appearances • The “Abnormal” Abdomen – Signs and hints

What are the INDICATIONS FOR ABDOMINAL X-RAY?
")
Indications • Pain (plus other symptoms – not really justifiable on it’s own? ) • BNO • Blood in: – Stool (malaena) – Urine (haematuria: frank=visible, microscopic=not) • Previous history of: – Abdominal surgery, pathology – Renal/Gall stones • • Abdominal distention Diarrhoea Nausea, Vomiting Foreign Body
 – “Making the best use")
Guidelines for Referral • Royal College of Radiologists (RCR) – “Making the best use of Clinical Radiology” or i. Refer RCR i. Refer guidelines for plain abdominal radiography; Clinical suspicion of perforation or obstruction Acute exacerbation of inflammatory bowel disease Palpable mass (specific circumstances) not often Constipation (specific circumstances) not often Acute and chronic pancreatitis Sharp/poisonous foreign body Smooth and small foreign body, e. g. , coin (specific circumstances) • Blunt or stab abdominal injury • •

Contraindications • Symptoms that would best be investigated with alternative imaging modalities: – Gallbladder, Liver, Pancreas – Ultrasound – Known renal history – CT, Nuclear Medicine (MAG 3, DMSA) – Perforation should be imaged with erect CXR! • Uninvestigated Symptoms that could be caused by PREGNANCY – Always make sure LMP is checked for abdominal imaging • Constipation with NO suspicion of obstruction

Now we’ve agreed why HOW AND WHEN?
 (most common) supine or erect")
Abdominal Views • A quick recap – Anteroposterior (AP) (most common) supine or erect – Posteroanterior (PA) – Lateral Decubitus – Upper abdominal image “renal area” or “cross-kidney” – Bladder views – Occasionally multiple abdomens for large patients or gross distention – Intravenous Urogram • Series of abdominal films pre and post contrast WHAT DO WE NEED TO SEE ON THE ABDOMINAL IMAGE?

Area of Interest • Simply put: • Diaphragm to symphysis pubis – Especially important with renal symptoms to fully include symph to exclude stones passed through to bladder • Lateral borders of abdomen – This means doing more than one film for acute patients to include all of the bowel

So What is a NORMAL ABDOMEN?


ORGANS - BOWEL LARGE stomach LARGE Bowel regions BOWEL GAS SMALL

Normal Stomach Pattern

Is this okay?

Fluid Level in Stomach ERECT ABDO

Normal Large Bowel Pattern Faecal Matter

Can you see the renal areas?
 for KUB Higher")
Well contrasted imaging helps How? Lower k. V (80 or less) for KUB Higher m. As (AEC compensation, manual exposures of 32 m. As+)

ORGANS - LARGE GALL BLADDER SPLEEN LIVER KIDNEYS BLADDER

OTHER STRUCTURES L 1 L 2 Psoas Muscles L 3 L 4 L 5

ABNORMAL ABDOMINAL X-RAYS BOWEL PATHOLOGY


Air in peritoneum stoma PNEUMOPERITONEUM/ACUTE PERFORATION

PERFORATION • Clinical guidelines state – AXR NOT INDICATED FOR PERFORATION – However this patient clearly has a stoma which has been compromised; either during the surgery or following – This would justify the AXR but an erect CXR would have been performed for completeness – Perforation is a SURGICAL EMERGENCY – can cause peritonitis which could be fatal

ERECT CHEST FOR ? PERFORATION AIR UNDER DIAPHRAGM


RIGLERS SIGN TRIANGULAR GAS POCKET Both sides of stomach wall and bowel wall visible – grossly distended stomach – PERFORATION/PNEUMOPERITONEUM


Small bowel pattern Surgical clips Artefacts? ? Embolisation coils SMALL BOWEL OBSTRUCTION

Other SBO signs • “string of pearls” • Small bubbles of air trapped in the valvulae of small bowel


LARGE BOWEL PATTERN LARGE BOWEL OBSTRUCTION


SIGMOID VOLVULUS Large bowel obstruction – sigmoid colon twists on itself COFFEE BEAN SIGN

Sigmoid Volvulus • Caused by long-term chronic constipation • More common in older patients and males • Can cause complete vascular disruption to bowel wall, obstruction and perforation • Perforation -> peritonitis ->danger


Intussusception

Intussusception • Most common medical emergency <2 yo ; 4 in 4000 probability, greater in boys • One layer of bowel slips over another • Causes swelling and bleeding, blockage of bowel • Serious cases can cause tissue death and loss of function; peritonitis!

ABNORMAL ABDOMINAL X-RAYS ORGAN PATHOLOGY


HEPATOMEGALY Enlarged Liver Sharp angle to lower border

Hepatomegaly Enlargement of the liver is usually caused by • Infections – Hepatitis – Glandular Fever (acute) – Cirrhosis • Tumours – – Metastases Liver carcinoma Leukaemia Lymphoma • Disease – congenital problems – drugs/alcohol


SPLENOMEGALY

Splenomegaly • Spleen enlarges slightly in normal function – however major enlargement may be caused by: – Dealing with major infection – Trauma – Tumours • Increased risk of rupture and major blood loss


Bra artefact Calcified gallstones Phlebolith in bladder


Air in stomach STAGHORN CALCULUS Complete obstruction of the renal pelvis Bladder phlebolith


RENAL CALCULUS

IVU


ABDOMINAL TOMOGRAM


Duplex Kidney Bifid Ureters

STONES! • Cause pain and obstruction of renal/biliary systems – Can be treated by surgical removal or laser fragmentation, lithotripsy or if small enough just monitored until they pass • Patients may undergo fluoroscopic procedures to treat these stones – ERCP – Retrograde Ureterogram – etc

ABDOMINAL PATHOLOGY OTHER PATHOLOGY


URETERIC STENT
 or retrograde (via retrograde ureterogram) • To")
URETERIC STENT • Installed antegrade (via nephrostomy) or retrograde (via retrograde ureterogram) • To release hydronephrosis caused by obstruction of the renal system – Stones – Pressure caused by disease


Gastric band Adjustment catheter And port


COIN

Ingested FBs • Can range from coins to button batteries, utensils, razorblades – the list is endless • Sharp FBs carry risk of perforation • Button battery acid can cause tissue necrosis – DANGER


Intrathecal Pump For Administering medication

Intrathecal pump • Small, surgically inserted pump • Used to direct small volumes of medication around the intrathecal space, around the spinal cord • Commonly used for – Chronic pain – Spasticity or displegia


ABDOMINAL AORTIC ANEURYSM

Aortic Aneurysm • Stretching and swelling of the muscle layers in the aorta (usually around 2. cm diameter) • Causing loss of blood pressure, pulsating feeling • Large aneurysms (5 cm or greater) are at risk of rupture, dissection internal bleeding and death. • Some can be treated depending on their location

VASCULAR STENT

Aortic Stent • Used to treat aneurysm • Deployed when aneurysms are not near arteries that could be occluded (renal, etc)
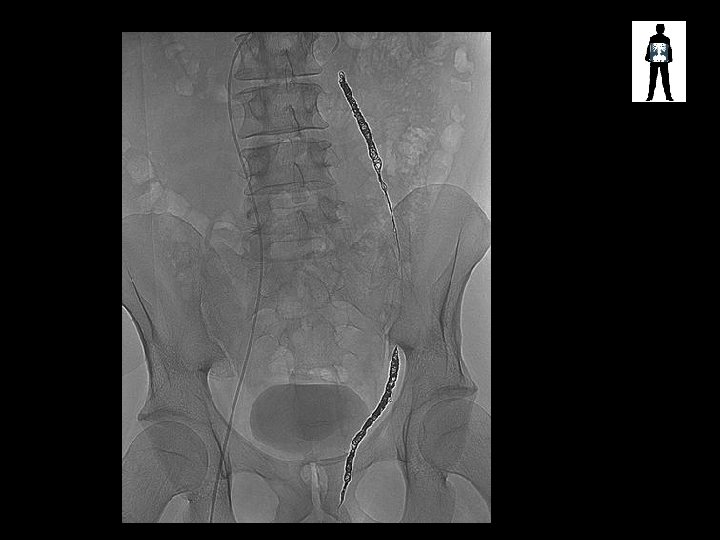

Varicocele Embolisation coils

Varicocele Embolisation Coils • Varicocele – enlarged scrotal vein – Causes pain, swelling, leads to infertility – Treated via embolization with coils or embolic fluid


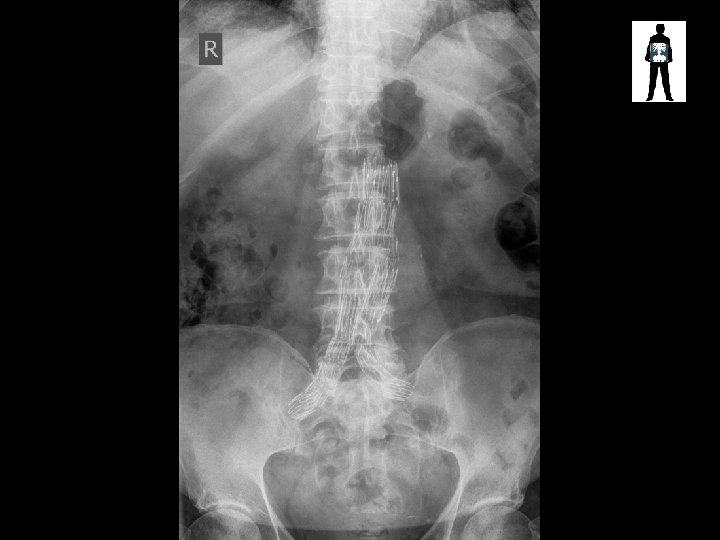
SURGICAL CLIP SPINAL FUSION SCREWS AND ROD


ORANGE

ANY QUESTIONS?

Elliott. J 9@Cardiff. ac. uk FURTHER INFORMATION
- Slides: 85