ABDOMINAL EXAMINATION BY Dr Sally Abed Lecturer Tropical

ABDOMINAL EXAMINATION BY Dr. Sally Abed Lecturer Tropical Medicine

ABDOMINAL EXAMINATION INSPECTION PALPATION PERCUSSION AUSCULTATION
 Quadrants (Clinical) 4")
Anatomy Regions (Anatomical) Quadrants (Clinical) 4

ABDOMEN: Inspection

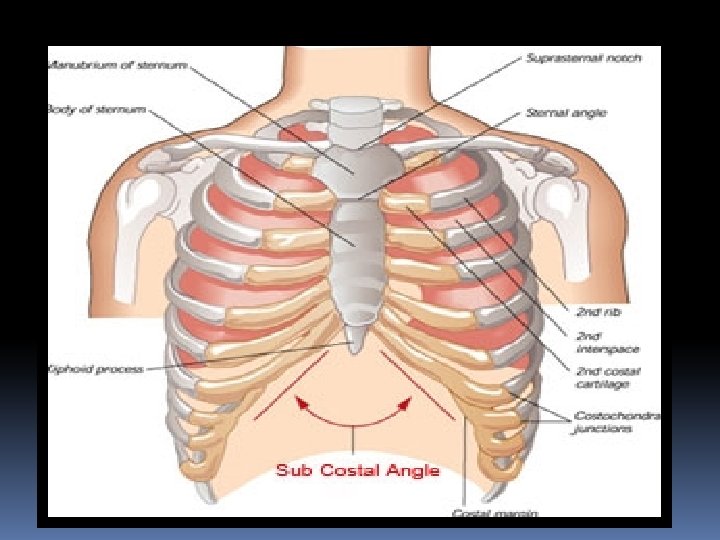
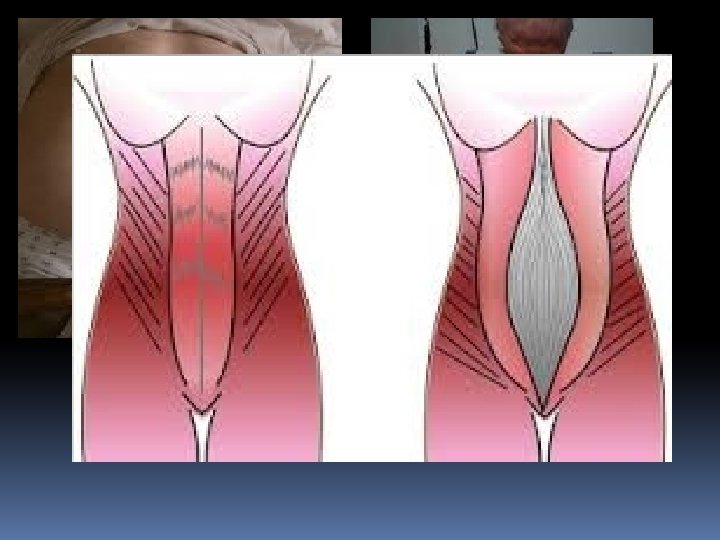
INSPECTION Mid line inspection 1 -Subcostal angle 2 -Epigastric pulsation 3 -Divercation of recti 4 -Umblicus 5 -Suprapubic hair distribution 6 -Hernial orifices Inspection of sides 1 -Contour of abdomen 2 - Dilated veins 3 - Skin 4 -Scars 5 - Movement with resp 6 -Visible peristalisis

MID LINE INSPECTION 1 -Subcostal angle causes of 2 -Epigastric pulsation causes 3 -Divercation of recti ? ? 4 -Umblicus - Site - Dilated veins - shape - Skin - Hernia - Discharge 5 -Suprapubic hair distribution 6 -Hernial orifices

 3 -")
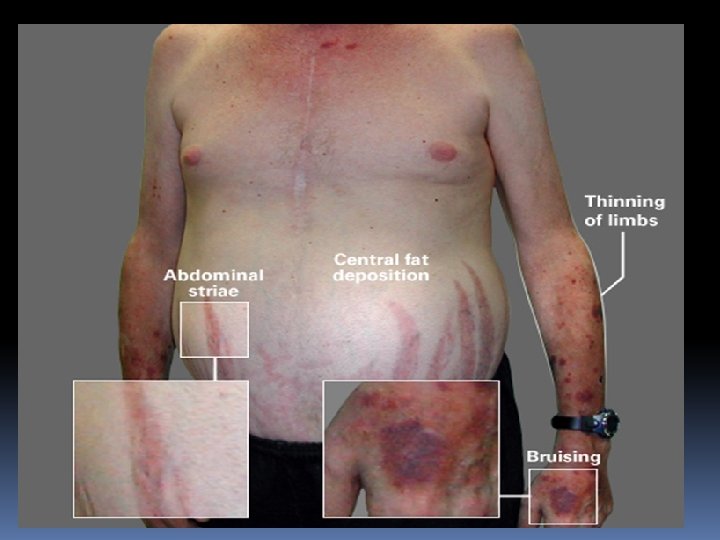
INSPECTION OF SIDES 1 -Contour of abdomen 2 - Collaterals (dilated veins) 3 - Skin abdominal wall -Striae, scratch marks, sinus& fistula -Pigmentation, purpura 4 -Scars Type, site, pigmentation, impulse on cough 5 - Movement with respiration 6 -Visible peristalsis

 Fat (obesity) Flatus and faeces Fluid")
Causes of abdominal enlargement ? Generalized: Fluid (ascites) Fat (obesity) Flatus and faeces Fluid in cyst (ovarian cyst) Fetus (pregnancy) Full bladder 2)Localized: Hernias → size ↑ with cough Masses in abdominal wall ( abscess & tumors) Enlargement of intra-abdominal organs
 1)Portal vein obstruction 1 -Site -Central around the umbilicus (caput medusa)")
Collaterals (dilated veins) 1)Portal vein obstruction 1 -Site -Central around the umbilicus (caput medusa) 2)IVC obstruction -Lateral in flanks and back 2 -Direction of -Away from filling umbilicus. From below upwards 3 -Oral glucose test Blood glucose in abd. wall veins > cubital vein Blood glucose in abd. wall veins = cubital vein


IVC obstruction

PALPATION

1. Ensure that your hands are warm 2. Stand on the patient’s right side 3. Help to position the patient 4. Ask whether the patient feels any pain before you start 5. Begin with superficial examination 6. Move in a systematic manner through the abdominal quadrants 7. Repeat palpation deeply.

PALPATION Superficial • Tenderness • Regidity • Masses Deep 1 - Liver 2 - Spleen 3 - Kidneys 4 - Gall bladder 5 - Colon

Normally Palpable Structures

PALPATION OF THE LIVER Technique of palpation: 1 - Upper border 2 - Lower border 3 - Liver span Comment on: 1 - Size 4 - Consistency 2 - Surface 5 - Tenderness 3 - Edge 6 - Pulsation

Liver Span
Infection: -Viral: Viral hepatitis , IMN, CMV -Bacterial: Brucellosis , T.")
Causes of hepatomegaly? 1)Infection: -Viral: Viral hepatitis , IMN, CMV -Bacterial: Brucellosis , T. B -Parasitic: Bilharziasis, Malaria , Fasciola 2)Congestion: -Rt side ht failure -Tricusbed valve disease -Constrictive pericarditis -Budd chiari syndrome -Veno-occlusive disease
Infiltration - Amyloidosis - Leukemia - Lymphoma 6)Neoplastic: - HCC - Metastasis 7)Miscellaneous: -Collagen")
3)Infiltration - Amyloidosis - Leukemia - Lymphoma 6)Neoplastic: - HCC - Metastasis 7)Miscellaneous: -Collagen disease -Congenital cysts

Causes of tender liver : 1 - Infection 2 - Congestion 3 - Cholestasis 4 - Infiltration 5 - Malignancy

PALPATION OF THE SPLEEN Technique of palpation - Usual method - Bimanual examination - Two handed method - Hooking method - Dipping method

132 -133: Palpation: Spleen (correctly - position, breaths, palpating deepest full inspiration, 1 hand under L side, 1 feeling) Palpation: Spleen (if not palpable, R lateral decubitus)

Right lateral decubitus
Infection: 1 -Viral: IMN, CMV 2 -Bacterial: Septecemia , Typhoid")
Causes of spenomegaly ? 1)Infection: 1 -Viral: IMN, CMV 2 -Bacterial: Septecemia , Typhoid fever , Brucellosis T. B , Syphilis 3 -Parasitic: Bilharziasis, Malaria, Leishmania 2)Congestion: (portal hypertension) 3)Infiltration -Amyloidosis -Sarcoidosis -Lipid storage disease -Leukemia- -Gaucher disease -Lymphoma
Blood disease: -Anemia 2 -Polycythemia -Myeloproliferative disease 5)Neoplastic: -Hemangioma -Sarcoma -Metastasis 6)Miscellaneous: -Collagen disease")
4)Blood disease: -Anemia 2 -Polycythemia -Myeloproliferative disease 5)Neoplastic: -Hemangioma -Sarcoma -Metastasis 6)Miscellaneous: -Collagen disease -SLE -Rh. artheritis

Grades of splenomegaly ? - Mild: Spleen just palpable under costal margin - Moderate: Spleen is palpable between costal margin and umbilicus - Huge : Spleen is palpable below the umbilicus

Causes of huge splenomegaly ? Bilharziasis Chronic malaria Kala azar Chronic myloid leukemia Hairy cell leukemia Myelofibrosis, myelosclerosis B- thalasemia Amyloidosis Gaucher, s disease

Causes of tender spleen ? 1 - Infection: - Septicemia - Infective endocardtis - Typhoid fever - Brucellosis - Acute malaria 3 - Infarction: (perisplenitis, splenic rub) 4 - Sickle cell anaemia 5 -Causes of huge splenomealy

PALPATION OF THE KIDNEY Bimanual palpation Causes of enlargement f the kidney? 1 - Hydronephrosis 2 - Pyonephrosis 3 - Polycystic kidney 4 - Tumour

135 -136: Palpation of Kidneys Right kidney (take a deep breath, capture kidney, exhale, slowly release kidney Left kidney (take a deep breath, capture kidney, exhale, slowly release kidney)

Splenic swelling 1 -Notch on anterior border (pathognomoni Kidney swelling -No notch; reniform in shape 2 -Hand cannot be -Can be insinuated ( ) swelling & costal margin &costal margin 3 -Does not fill renal angle -Fills the renal angle 4 -Dull on percussion & -Percussion above swelling continuous with splenic → band of colonic dullness resonance anteriorly 5 -Moves with respiration 6 -No posterior ballotment -Posterior ballotment

Percussion

PERCUSSION Ascites • Minimal ascites • Moderate ascites • Tense ascites Abdominal organs • Liver • Spleen • Urinary bladder • Any palpable mass


Percussion: Liver span The liver span is estimated by percussion. Remember that it is easier to hear the change from resonance to dullness – so proceed with percussion from areas of resonance to areas of dullness. Upper border: In the midclavicular line start percussing in the chest moving down towards the abdomen about ½ to 1 cm at a time. Note where the percussion notes change from resonate to dull. Lower border: In the midclavicular line begin percussion below the unbillicus and proceed upward until dullness is encounter. The distance between the two areas where dullness is first encountered is the liver span. Liver span is normally 6 to 12 cm in the midclavicular line.

PUDDLE SIGN JAMA 1992; 267: 2645 -2648

Premature ascites: Dif: Ascites in cirrhotic patients before shrunken liver Causes: Reversible Not reversible 1 -Hematemsis & melena 1 -Malignant 2 -Severe vomiting & diarrhea 2 -T. B peritonitis 4 -Intercurrent infection 3 -B. nephropathy 5 -Old anti-bilharzial

Ascites precox: Dif: Ascites before edema lower limb in cardiac patients Causes: 1 -T. R 2 -Pericardial effusion 3 -Constrictive pericarditis

PERCUSSION OF THE SPLEEN 1 - Percussion of traube’s area 2 - Castell’s method 3 - Nixon’s method

1 2 1 -Nixon's Method: Place the patient in the right lateral decubitus position. Initiate percussion half-way along the costal margin and percuss cephalad in a line perpendicular to the costal margin. Dullness of >8 cm suggests splenomegaly. 2 -Castell's Sign (in Traube's Space): in supine percuss in the lowest intercostal space in the left-anterior axillary line in full expiration and inspiration. Splenomegaly is suggested when the percussion is dull or becomes dull on inspiration.

Nixon method

Traubs area

Traub’s area: Area of tympanetic resonance over fundus of the stomach Causes of dullness in traub’s area: 1 -From above: Lt pleural eff. , Pericardial eff. 2 -From left : Splenomegally 3 -From Right : Hepatomegally 4 -From below: -Full stomach -Subpherinic abcess -Gastric tumour -Retroperitoneal neoplasm -Ascites -Complete situs inversus -Pregnancy

AUSCULTATION

Intestinal sounds Vascular sound -Arterial bruit -Venous hum Friction rub -Splenic rub -Hepatic rub Succusion splash Minimal ascites (puddle sign) Lower border of liver (scratching method)

Auscultate Bowel Sounds

Auscultate Vascular Sounds

- Slides: 54