ABDOMEN I ANTEROLATERAL ABDOMINAL WALL Abdomen boundaries Superiorly

ABDOMEN I: ANTEROLATERAL ABDOMINAL WALL
 • Xiphoid • Costal cartilages Sides/walls:")
Abdomen boundaries: Superiorly: • Diaphragm (T 10 roof) • Xiphoid • Costal cartilages Sides/walls: • Musculotendinous (flank mm. ) • Lumbar vertebral bodies & trans. processes • False ribs (11 -12) Inferior • False pelvis • Superior pelvic opening (pelvic brim) Note: • Angle of abdominopelvic cavity • One continuous cavity: abdominal organs can become pelvic and vice versa (bladder, intestine) • changes @ sup. pelvic opening
![HIP BONES (2) [os coxae, coxal bones] Iliac Crest ILIUM Arcuate line of the](http://slidetodoc.com/presentation_image_h2/4e74b3c6ea63b6ba527a8dffb299a2f3/image-3.jpg "HIP BONES (2) [os coxae, coxal bones] Iliac Crest ILIUM Arcuate line of the")
HIP BONES (2) [os coxae, coxal bones] Iliac Crest ILIUM Arcuate line of the ilium Pectineal line (pectin pubis) Auricular surface (for S-I jnt. ) Pu Ra bic m us PUBIS ISCHIUM Pubic symphysis -classic fibrocartilaginous jnt.
 Lateral border of rectus m. intersects costal cartilage RIGHT EPIGASTRIC HYPOCHONDRIACEPIGASTRIC")
MIDCLAVICULAR PLANES (R&L) Lateral border of rectus m. intersects costal cartilage RIGHT EPIGASTRIC HYPOCHONDRIACEPIGASTRIC LEFT HYPOCHONDRIAC TRANSPYLORIC PLANE RIGHT LUMBAR UMBILICAL LEFT LUMBAR INTERTUBERCULAR PLANE RIGHT INGUINAL HYPOGASTRIC LEFT INGUINAL UPPER RIGHT LOWER RIGHT UPPER LEFT LOWER LEFT
 Camper’s fascia")
SUPERFICIAL FASCIA OF THE ABDOMINAL WALL Fascia lata (deep fascia of thigh) Camper’s fascia -fatty layer Scarpa’s fascia -membranous layer -visible on CT -can hold suture Position of Penis Colles’ fascia -membranous layer Position of Scrotum

Camper’s fascia
 Fascia Colles’ fascia Dartos fascia -male only -smooth muscle")
Scarpa’s fascia Superficial Penile (Clitoral♀) Fascia Colles’ fascia Dartos fascia -male only -smooth muscle mixed in -gives scrotum a “raisin skin” appearance

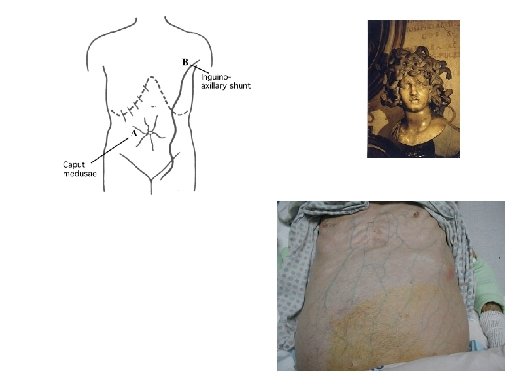
ABDOMINAL WALL VEINS lateral thoracic vein drains to axillary vein portal vein in porta hepatis lumbar veins paraumbilical veins (follow falciform ligament in liver and extend onto anterior abdominal wall) superficial epigastric vein drains to great saphenous vein (then femoral)
 muscles Intercostal/Subcostal/L 1")
ABDOMINAL WALL ARTERIES/NERVES supplies rectus abdominus m. supplies lateral wall (flank) muscles Intercostal/Subcostal/L 1 nerves: Supply segmental motor and sensory innervation to abdominal wall Subcostal Nerve Superficial Inguinal Ring sensation to mons pubis/upper groin thru inguinal canal sensation to ext. genitalia supplies rectus abdominus m.
 level is")
LYMPH DRAINAGE ON ANTEROLATERAL ABDOMINAL WALL Axillary Lymph Nodes T 10 (umbillicus) level is “watershed” line y Superficial Inguinal Lymph Nodes
 -thickening")
anterior sacroiliac lig. -nearly motionless pectineal lig. (a. k. a. Cooper’s lig. ) -thickening of periosteum -can suture to it (strong) inguinal lig. (ASIS→pub. tubercle) lacunar lig. (inguinal lig. →pectineal lig. )

EXTERNAL OBLIQUE • • • Outermost flank mm. Lateral & posterior = muscular Anterior & inferior = tendinous Fibers project inferomedially Originates from ribs 5 -12 Inserts on: • • • Inguinal Ligament Antimere in midline (linea alba) Pubic symphysis (superior edge) Pubic tubercle NOT along pubic crest Iliac crest Superficial Inguinal Ring Pubic Tubercle

INTERNAL OBLIQUE • • • middle flank mm. Lateral = muscular Anterior = tendinous Fibers project superomedially Originates from: • thoracolumbar fascia • Iliac crest • Inguinal lig. Thoracolumbar Fascia Inguinal Ligament • Inserts on: • • Antimere in midline (linea alba) Lower ribs & costal cart. Pubic symphysis (superior edge) Pubic crest & beginning of pectineal line Internal Oblique contribution to the CONJOINT TENDON -fusion of internal obl. and transversus abd. aponeuroses along pubic crest & portion of pectineal line

TRANSVERSUS ABDOMINUS Thoracolumbar Fascia Inguinal Ligament • • • innermost flank mm. Lateral = muscular Anterior = tendinous Fibers project transversely Originates from: • • Thoracolumbar fascia Iliac crest Inguinal lig. Costal cartilages Arcuate Line of the Abdominal Wall -a slit in the aponeurosis that allows rectus abd. to pass • Inserts on: • Antimere in midline (linea alba) • Pubic symphysis (superior edge) • Pubic crest & beginning of pectineal line Transversus Abdominus contribution to the CONJOINT TENDON
 tendinous insertions Linea semilunaris • “strap”")
RECTUS ABDOMINUS position of gall bladder (transpyloric plane) tendinous insertions Linea semilunaris • “strap” mm. • Tendinous insertions Linea Alba =multiple muscle bellies -fusion raphe btwn. R & L aponeuroses from flank mm. • Fibers project superoinferiorly • Originates from: • Costal cart. of ribs 5 -8 • Sternum/xiphoid • Inserts on: Mc. Burney’s point: (2/3 rds distance from umbillicus to ASIS) • Pubic crest • Pubic symphysis (superior -approx. position of edge) appendix

linea alba Mc. Burney’s Point =appendix linea semilunaris Function of abdominal wall muscles (flank mm. and rectus): ·Stabilize the trunk ·Flexion ·Lateral flexion ·Torsion ·Abdominal compression (working with diaphragm)

ORGANIZATION OF RECTUS SHEATH External Oblique Internal Oblique Transversus Abdominus rectus sheath Rectus Abdominus Tendinous covering around rectus muscles, derived from flank mm. aponeuroses Arcuate Line of Abdominal Wall

ABOVE ARCUATE LINE BELOW ARCUATE LINE RECTUS Transversalis fascia Peritoneum
 houses median umbilical ligament (urachus remnant)")
DEEP SURFACE OF ANTERIOR WALL Median fold (1) houses median umbilical ligament (urachus remnant) Falciform lig. • Separates liver into R & L anatomical lobes • Bottom free edge houses paraumbilical veins and round lig. of the liver Medial folds (2) house obliterated umbilical arteries Lateral folds (2) houses inferior epigastric vessels

INGUINAL CANAL deep inguinal ring -hole in transversalis fascia inguinal canal intercrural fibers (prevents “banana-peeling”) lateral crus medial crus INGUINAL CANAL CONTENTS: ·Ilioinguinal nerve superficial inguinal ring -hole in external obl. aponeurosis ·Spermatic cord (♂) ·Round ligament of the uterus (♀)

testicular blood vessels vas deferens BLADDER spermatic cord

HESSELBACH’S TRIANGLE – SEEN FROM DEEP SURFACE OF ANDOMINAL WALL Borders: medial = rectus abdominus inferior = inguinal ligament lateral = inferior epigastric artery Deep ring: always lateral to triangle superficial ring: overlaps triangle

EPIDIDYMIS Head Efferent ductules Testicular a. Body Tail Pampiniform plexus Sac made from peritoneum that covers the anterior, lateral, and inferior portions of the testis

SPERMATIC CORD Vas deferens Genital branch of genitofemoral nerve External spermatic fascia Cremasteric fascia (with cremaster muscle) Internal spermatic fascia Pampiniform plexus Testicular a.

SPERMATOCELES • Caused by cysts in the rete testis, efferent ductules, and head of epididymis. • Cysts are distended with milky fluid that contains sperm. • Asymptomatic except when large, causing testicular discomfort. • Can be transilluminated (e. g. , flashlight) • Causes: – Epididymitis (infection) – tubule diverticula that swell over time from spermatogenesis

• • • TESTICULAR TORSION Spermatic cord gets twisted around the blood vessels, cutting off testicle's blood supply, Most common in 12 -18 yr olds. Usually caused by sportsrelated groin injury: cremaster spasms and twists testis. Immediate pain. Requires immediate treatment to save testis (untwist and suture to scrotal wall). TESTICULAR VARICOCELES (BAG OF WORMS) Reduced venous return from testes via pampiniform plexus. Results in enlargement of the veins, looks and feels like a “bag of worms. ” More common on left side because of left testicular vein drainage. Frequently occurs in runners neglecting proper support (bouncing). Usually develops slowly; usually no symptoms. Common cause of infertility in men.

HYDROCELES NORMAL CONGENITAL Hydrocele: Accumulation of serous fluid around one or both testicles (within tunica vaginalis or processus vaginalis ) that causes the scrotum or groin area to swell. FUNICULAR VAGINAL
 -deep ring fails")
INDIRECT INGUINAL HERNIA -enters thru deep ring (lateral to Hesselbach’s Δ) -deep ring fails to seal off -can proceed all the way thru inguinal canal to scrotum or labium majus

INDIRECT HERNIA -enters wall lateral to inf epigastric a. DIRECT HERNIA -medial to inf epigas. art -failure of the conjoint tendon

2%
- Slides: 31