ABCDE Approach ALS Metaxia Bareka Anesthesiologist ERC Course

ABCDE Approach ALS Metaxia Bareka Anesthesiologist ERC Course Organizer, Course Director

ABCDE Approach Underlying principles: �Complete initial assessment �Treat life-threatening problems �Reassessment �Assess effects of treatment/interventions �Call for help early

A irway B reathing C irculation D isability E xposure

Initial assessment �Personal safety �Patient responsiveness �First impression Movement Pulse Respiratory effort Temperature

Α: Airway

Α Causes of airway obstruction �CNS depression �Infection �Blood �Inflammation �Vomit �Laryngospasm �Foreign body �Bronchospasm �Trauma

Α Recognition of airway obstruction �Talking �Difficulty breathing, distressed, choking �Shortness of breath �Noisy breathing Stridor, wheeze, gurgling �See-saw respiratory pattern, accessory muscles

Α Treatment of airway obstruction �Airway opening Head tilt, chin lift, jaw thrust �Simple adjuncts �Advanced techniques e. g. LMA, tracheal tube �Oxygen �Early Caponography

A: Airway �Protection of Cervical Spine �Ο 2

B: Breathing

Β Causes of breathing problems � Decreased respiratory drive CNS depression � Decreased respiratory effort Muscle weakness Nerve damage Restrictive chest defect Pain from fractured ribs � Lung disorders Pneumothorax Haemothorax Infection Acute exacerbation COPD Asthma Pulmonary embolus ARDS

Β Recognition of breathing problems �Look Respiratory distress, accessory muscles, cyanosis, respiratory rate, chest deformity, conscious level �Listen Noisy breathing, breath sounds �Feel Expansion, percussion, tracheal position

Β Treatment of breathing problems �Airway �Oxygen �Treat underlying cause e. g. drain pneumothorax �Support breathing if inadequate e. g. ventilate with bag-mask �Establish continuous monitoring (Sp. O 2, respiratory rate)

Β B: Breathing �Sp. O 2 �Respiratory Rate �Look �Percussion �Auscultation �Feel �Position of the trachea

C: Circulation

C Causes of circulation problems � Primary Acute coronary syndromes Arrhythmias Hypertensive heart disease Valve disease Hereditary cardiac diseases (Drugs) (Electrolyte/acid base abnormalities) � Secondary Asphyxia Hypoxaemia Blood loss Hypothermia Septic shock (Drugs) (Electrolyte/acid base abnormalities

C Recognition of circulation problems �Look at the patient �Pulse - tachycardia, bradycardia �Peripheral perfusion - capillary refill time �Blood pressure �Organ perfusion Chest pain, mental state, urine output �Bleeding, fluid losses �Record and document an ECG

C Treatment of circulation problems �Airway, Breathing �Oxygen �IV/IO access, take bloods �Establish ECG monitoring �Treat cause �Fluid challenge �Haemodynamic monitoring �Inotropes/vasopressors �Aspirin/nitrates/oxygen (if appropriate) and morphine for acute coronary syndrome

D: Disability

D Recognition �AVPU or GCS �Pupils Size Equality Responsiveness to light �Neurological deficits �Blood glucose


D Κλίμακα AVPU �A: Alert Awake, conscious �V: Voice Reaction to vocal stimuli �P: Pain Reaction to painful stimuli �U: Unresponsive No response

D Treatment �ABC �Ο 2 �Treat underlying cause �Blood glucose If < 4 mmol l-1 give glucose �Consider lateral position �Check drug chart

Ε: Exposure

E Exposure �Remove clothes to enable examination e. g. injuries, bleeding, rashes �Avoid heat loss �Maintain dignity


A: Airway �Secure / obstructed / in danger �Ο 2 �Cervical spine

B: Breathing �Respiratory Rate �Auscultation �Quality of breathing: Depth of breathing Type of breathing �Percussion �Sp. O 2 �Look: Deformities Chest expansion Jugular veins �Feel: Position of the tracheia Subcutaneous emphysema

C: Circulation � Pulse: centrally + peripherally � Blood pressure � CRT � Auscultation of the heart � Iv access � Take blood: Full blood count Biochemistry Coagulation Blood cross match Cardiac enzymes - Troponin Blood gases � 12 lead EVG � Monitor � Fluids � Control hemorrhage � Urine output � Color – temperature of extremities � Check for signs of heart failure

D: Disability �Conscious level AVPU ή GCS �Pupils Size Equality Responsiveness to light �Neurological deficit �Blood sugar �Substances intake

E: Exposure �Look: Ecchymosis Petecheia Bruises Rashes Oedema �Temperature �Enviroment �Call the expert

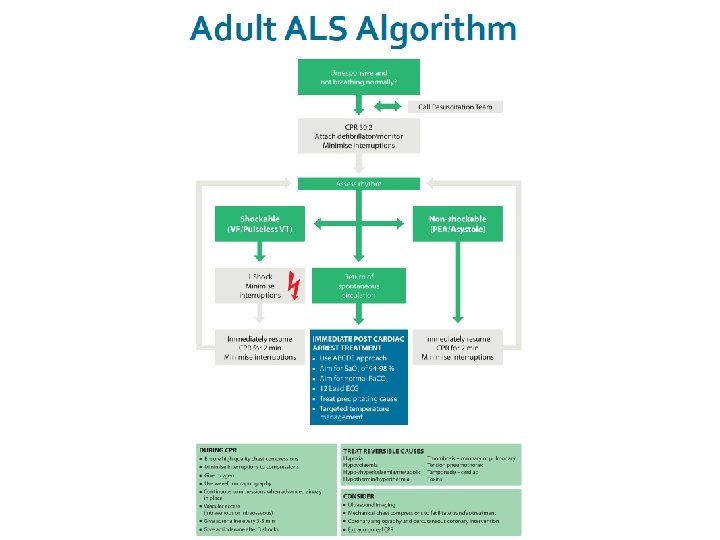
ALS Algorithm

Learning outcomes �The ALS algorithm �Importance of high quality chest compressions �Treatment of shockable and non-shockable rhythms �Administration of drugs during cardiac arrest �Potentially reversible causes of cardiac arrest �Role of resuscitation team

Confirmation of cardiac arrest �Patient response �Open airway �Check for normal breathing �Check circulation

Confirmation of cardiac arrest

 � Bizarre irregular waveform � No recognisable QRS complexes � Random frequency")
Shockable (VF) � Bizarre irregular waveform � No recognisable QRS complexes � Random frequency and amplitude � Uncoordinated electrical activity � Coarse/fine � Exclude artefact Movement Electrical interference
 � Monomorphic VT – Broad complex rythm – Rapif rate – Constant")
Shockable (VT) � Monomorphic VT – Broad complex rythm – Rapif rate – Constant QRS morphology � Polymorphic VT – Torsade de pointes
")
Shockable (VF/VT)
")
Shockable (VT)
")
Shockable (VF/VT)
")
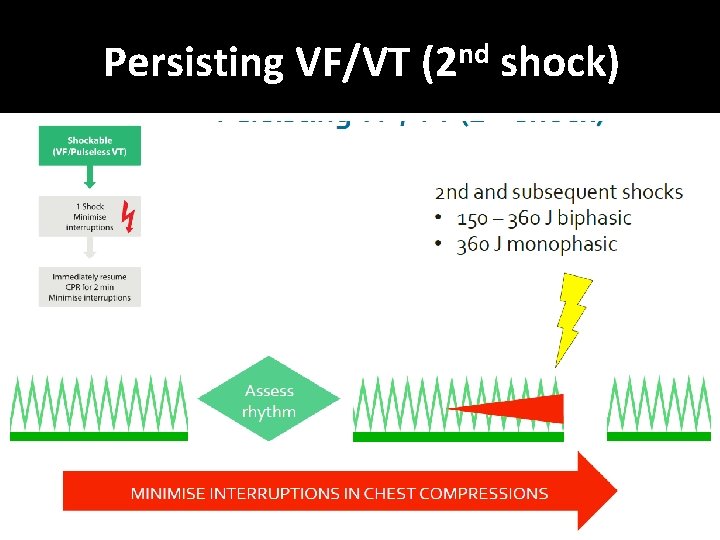
Shockable (VF/VT)
")
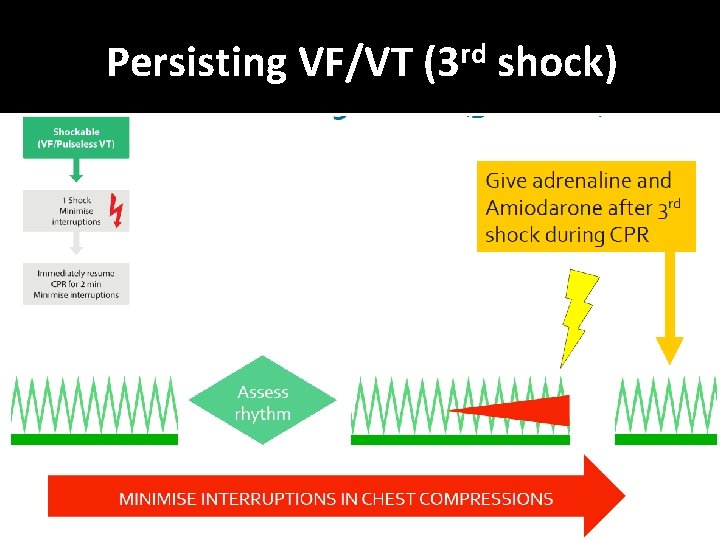
Shockable (VF/VT)
 �If unsure, deliver")
Defibrillation energies � 150 – 360 J biphasic (360 J monophasic) �If unsure, deliver highest available energy �DO NOT DELAY SHOCK

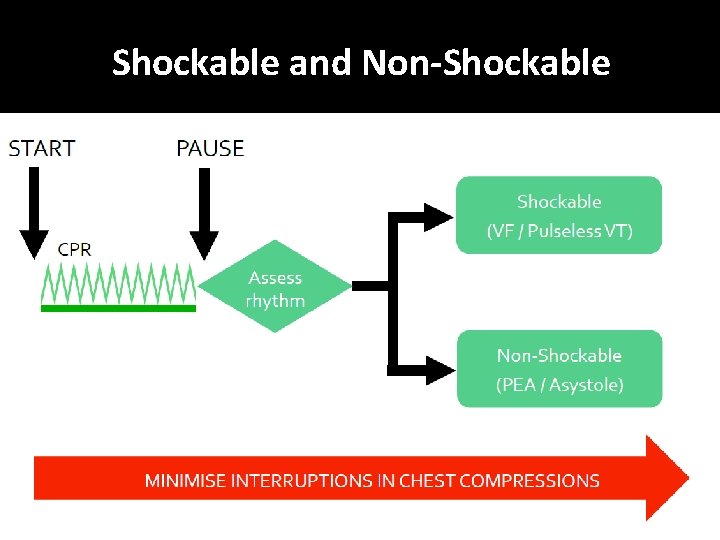
Non-Shockable
 � Absent ventricular (QRS) activity � Atrial activity (P waves) may persist")
Non-Shockable (Asystole) � Absent ventricular (QRS) activity � Atrial activity (P waves) may persist � Rarely a straight line trace � Adrenaline 1 mg IV then every 3 -5 min
 �Clinical features of cardiac arrest �ECG normally associated with an")
Non-Shockable (Pulseless Electrical Activity) �Clinical features of cardiac arrest �ECG normally associated with an output �Adrenaline 1 mg IV then every 3 -5 min

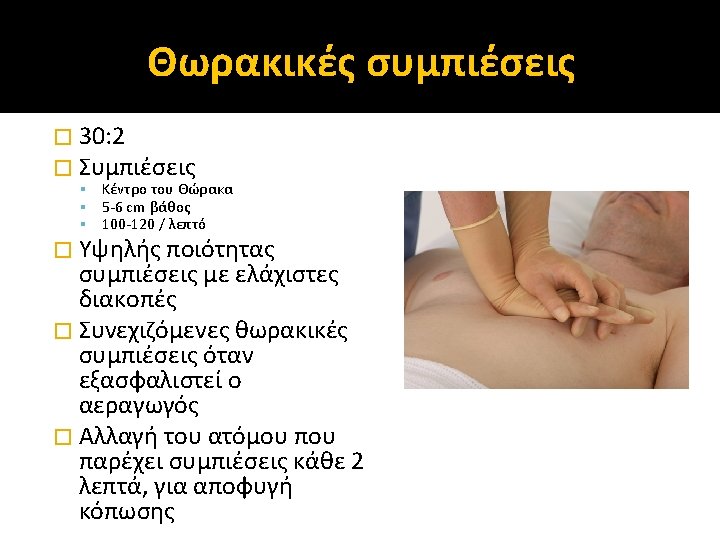
During CPR

Airway and ventilation �Secure airway: Supraglottic airway device e. g. LMA, LT, i-gel Tracheal tube �Do not attempt intubation unless trained and competent to do so �Once airway secured, if possible, do not interrupt chest compressions for ventilation �Avoid hyperventilation �Capnography

Vascular access � Peripheral versus central veins � Intraosseous

Reversible Causes

Hypoxia � Ensure patent airway � Give high-flow supplemental oxygen � Avoid hyperventilation

Hypovolaemia � Seek evidence of hypovolaemia History Examination • Internal haemorrhage • External haemorrhage • Check surgical drains � Control haemorrhage � If hypovolaemia suspected give intravenous fluids

Hypo/hyperkalaemia and metabolic disorders � Near patient testing for K+ and glucose � Check latest laboratory results � Hyperkalaemia Calcium chloride Insulin/dextrose � Hypokalaemia/ Hypomagnesaemia Electrolyte supplementation

Hypothermia � Rare if patient is an in- patient � Use low reading thermometer � Treat with active rewarming techniques � Consider cardiopulmonary bypass

Tension pneumothorax � Check tube position if intubated � Clinical signs Decreased breath sounds Hyper-resonant percussion note Tracheal deviation � Initial treatment with needle decompression or thoracostomy

Tamponade, cardiac � Difficult to diagnose without echocardiography � Consider if penetrating chest trauma or after cardiac surgery � Treat with needle pericardiocentesis or resuscitative thoracotomy

Toxins � Rare unless evidence of deliberate overdose � Review drug chart

Thrombosis � If high clinical probability for PE consider fibrinolytic therapy � If fibrinolytic therapy given continue CPR for up to 60 -90 min before discontinuing resuscitation

Ultrasound � In skilled hands may identify reversible causes � Obtain images during rhythm checks � Do not interrupt CPR

Immediate post-cardiac arrest treatment

Resuscitation team � Roles planned in advance � Identify team leader � Importance of non- technical skills Task management Team working Situational awareness Decision making � Structured communication


- Slides: 70