A Treating Docs View of Treating Docs By

”A Treating Doc’s View of Treating Docs” By Zachary A. Kordik, M. D. IAEAPE Annual Conference – Chicago, IL October 28, 2016

Affiliations v Rush University Medical Center v Hazelden Betty Ford Foundation v Foundations Recovery Network I have received no funding or sponsorship from any commercial entity in regards to this presentation.

Objectives 1. List and describe risks specific to certain high accountability professions and specialties. 2. Navigate barriers in identifying and recommending appropriate treatment for professionals. 3. Recognize the need, methods, and resources for professional treatment and advocacy in returning to work.

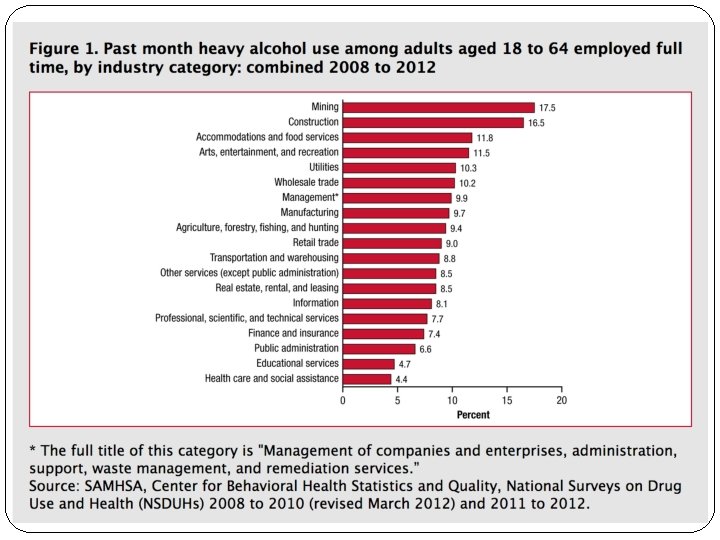
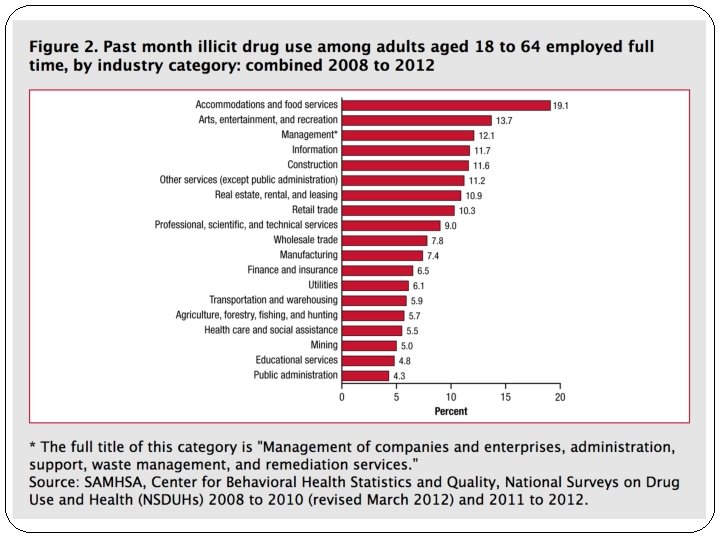
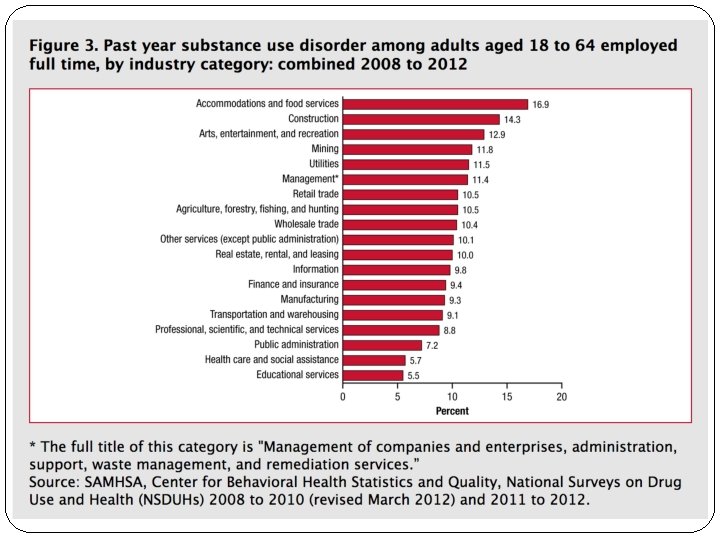
Substance Abuse by Industry “Substance Use and Substance Use Disorder by Industry” �Published by SAMHSA most recently April 16, 2015 �Data collected between 2008 and 2012 by the National Survey on Drug Use and Health (NSDUH) �Combined data from 2008 to 2012 indicate that an annual average of 8. 7 percent of full-time workers aged 18 to 64 used alcohol heavily in the past month, 8. 6 percent used illicit drugs in the past month, and 9. 5 percent were dependent on or abused alcohol or illicit drugs in the past year.

Physician Impairment �When assessing possible impairment of a physician two things must be weighed: Health of the physician Vs. Safety of the public

Physician Impairment �When assessing possible impairment of a physician two things must be weighed: Health of the physician Vs. Safety of the public

Physician Impairment �When assessing possible impairment of a physician two things must be weighed: Health of the physician Vs. Safety of the public (This is how most media, governments, and the public in general will see this balance. )
: �“Any physical, mental, or behavioral disorder that interferes with the")
Definitions Physician Impairment (AMA): �“Any physical, mental, or behavioral disorder that interferes with the physician’s ability to engage safely in professional activities. ”
: �“Any physical, mental, or behavioral disorder that interferes with the")
Definitions Physician Impairment (AMA): �“Any physical, mental, or behavioral disorder that interferes with the physician’s ability to engage safely in professional activities. ” �Can be a result of: Mental disorder 2. Physical illness or condition 3. Substance related disorder 1.
: �“Any physical, mental, or behavioral disorder that interferes with the")
Definitions Physician Impairment (AMA): �“Any physical, mental, or behavioral disorder that interferes with the physician’s ability to engage safely in professional activities. ” �Can be a result of: Mental disorder 2. Physical illness or condition 3. Substance related disorder 1. � Illness does not, per se, constitute impairment.
: �“A style of interaction with physicians, hospital personnel, patients,")
Definitions Disruptive Physician Behavior (AMA): �“A style of interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care. ”
: �“A style of interaction with physicians, hospital personnel, patients,")
Definitions Disruptive Physician Behavior (AMA): �“A style of interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care. ” �Behavior that is exhibited as a pattern
: �“A style of interaction with physicians, hospital personnel, patients,")
Definitions Disruptive Physician Behavior (AMA): �“A style of interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care. ” �Behavior that is exhibited as a pattern �Can include words, attitudes, and actions
: �“A style of interaction with physicians, hospital personnel, patients,")
Definitions Disruptive Physician Behavior (AMA): �“A style of interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care. ” �Behavior that is exhibited as a pattern �Can include words, attitudes, and actions �Potential to interfere with quality healthcare
: �“A style of interaction with physicians, hospital personnel, patients,")
Definitions Disruptive Physician Behavior (AMA): �“A style of interaction with physicians, hospital personnel, patients, family members, or others that interferes with patient care. ” �Behavior that is exhibited as a pattern �Can include words, attitudes, and actions �Potential to interfere with quality healthcare �Is a descriptive label, not a diagnosis

Physician Impairment �Estimates suggest that approximately 15% of physicians will be impaired at some point in their careers.

Physician Impairment �Estimates suggest that approximately 15% of physicians will be impaired at some point in their careers. �The leading cause of physician impairment is chemical dependence.
 �Substance d/o divided into two separate diagnoses �Dependence")
DSM-IV vs. DSM-V DSM-IV (1994 -2013) �Substance d/o divided into two separate diagnoses �Dependence – “dependence syndrome” �Abuse – social and interpersonal consequences of heavy use �Dependence above abuse in a hierarchy �Abuse should not be diagnosed with dependence was present

DSM-IV vs. DSM-V

DSM Criteria DSM-5: Alcohol/Substance Use Disorders �Specifiers: �Mild – presence of 2 -3 symptoms �Moderate – presence of 4 -5 symptoms �Severe – presence of 6 or more symptoms

DSM Criteria DSM-5: Alcohol/Substance Use Disorders �If full criteria for substance use disorder were previously met: �In early remission – no criteria* met for 3 -12 months �In sustained remission – no criteria* for > 12 months *with the exception of “craving, or a strong desire to use”

Chemical Dependency �Alcohol is the most commonly abused substance among physicians �Alcohol use disorders are no more common among physicians than similarly matched controls

Chemical Dependency �Alcohol is the most commonly abused substance among physicians �Alcohol use disorders are no more common among physicians than similarly matched controls �Physicians have higher rates of abuse of prescription drugs �Physician misuse of benzodiazepines and opioids are up to 5 X higher than in age matched populations

Chemical Dependency Possible reasons for higher rates of physician Rx drug abuse:

Chemical Dependency Possible reasons for higher rates of physician Rx drug abuse: 1. Easy access to these prescriptions/drugs

Chemical Dependency Possible reasons for higher rates of physician Rx drug abuse: 1. Easy access to these prescriptions/drugs 2. Familiarity with prescription drugs

Chemical Dependency Possible reasons for higher rates of physician Rx drug abuse: 1. Easy access to these prescriptions/drugs 2. Familiarity with prescription drugs 3. Overconfidence about drug use

Chemical Dependency Substances being abused by physicians in treatment: Drug of Abuse Percent Alcohol 39. 5 Opioids 33. 9 Cocaine 11. 9 Sedatives 3. 7 Marijuana 2. 8 Inhalants 1. 8 Amphetamines 1. 8 Other 4. 6

Chemical Dependency Specialty Percent

Chemical Dependency Specialty Anesthesiology Percent

Chemical Dependency Specialty Anesthesiology ER Percent

Chemical Dependency Specialty* Percent Anesthesiology 21 ER 18 Surgery 6 Family Medicine 6 OB/GYN 6 Radiology 6 Pathology 6 Neurology 3 Psychiatry 3 *Percentage of total number of 109 physicians in

Mental Illness Comorbidities �Physician substance abuse is associated with increased risk of suicide.

Mental Illness Comorbidities �Physician substance abuse is associated with increased risk of suicide. �Suicide rates are 40% higher in male physicians than age-matched peers.

Mental Illness Comorbidities �Physician substance abuse is associated with increased risk of suicide. �Suicide rates are 40% higher in male physicians than age-matched peers. �Suicide rates are 130% higher in female physicians than age-matched peers.

Mental Illness Comorbidities �Physician substance abuse is associated with increased risk of suicide. �Suicide rates are 40% higher in male physicians than age-matched peers. �Suicide rates are 130% higher in female physicians than age-matched peers. �Mental health problems that began before medical school may worsen during training.

Identifying Physician Impairment �Colleagues must play a role in the identification of impaired physicians.

Identifying Physician Impairment �Colleagues must play a role in the identification of impaired physicians. AMA Code of Medical Ethics – informs physicians they have an ethical obligation to report impaired, incompetent, and unethical colleagues.

Identifying Physician Impairment �Colleagues must play a role in the identification of impaired physicians. AMA Code of Medical Ethics – informs physicians they have an ethical obligation to report impaired, incompetent, and unethical colleagues. �Many states allow for this to be done anonymously.

Treatment for Impaired Physician

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition �Friends, family, or colleagues

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition �Friends, family, or colleagues �Employer/Supervisor

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition �Friends, family, or colleagues �Employer/Supervisor �EAP

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition �Friends, family, or colleagues �Employer/Supervisor �EAP �Medical board

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment �Self-recognition �Friends, family, or colleagues �Employer/Supervisor �EAP �Medical board �Legal entity

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment �Detoxificaton - treatment for withdrawal

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment �Detoxificaton - treatment for withdrawal �Professionals treatment program – PHP/IOP: 6 -8 weeks �Group therapy and support �Individual counseling �Education �MAT – Medication Assisted Treatment

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment �Detoxificaton - treatment for withdrawal �Professionals treatment program – PHP/IOP: 6 -8 weeks �Group therapy and support �Individual counseling �Education �MAT – Medication Assisted Treatment �Consider sober living residence

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare �Caduceus contract – requirements of aftercare for advocacy

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare �Caduceus contract – requirements of aftercare for advocacy �Continuing care group – weekly for 1 -2 years

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare �Caduceus contract – requirements of aftercare for advocacy �Continuing care group – weekly for 1 -2 years �Monitoring – random urine screens for 2 -5 years

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare �Caduceus contract – requirements of aftercare for advocacy �Continuing care group – weekly for 1 -2 years �Monitoring – random urine screens for 2 -5 years �Return to work – determine when, how, in what role, and with any restrictions

Treatment for Impaired Physician Step 1: Recognition of impairment and referral for treatment Step 2: Treatment Step 3: Aftercare �Caduceus contract – requirements of aftercare for advocacy �Continuing care group – weekly for 1 -2 years �Monitoring – random urine screens for 2 -5 years �Return to work – determine when, how, in what role, and with any restrictions �May include specific requirements of employer or medical board

To Report or Not To Report… Does an impaired physician have to report to the Board?

To Report or Not To Report… Does an impaired physician have to report to the Board? �Yes, will likely eventually have to report to the Board.

To Report or Not To Report… Does an impaired physician have to report to the Board? �Yes, will likely eventually have to report to the Board. A better question is…

To Report or Not To Report… Does an impaired physician have to report to the Board? �Yes, will likely eventually have to report to the Board. A better question is… When should an impaired physician report to the Board?

To Report or Not To Report… Does an impaired physician have to report to the Board? �Yes, will likely eventually have to report to the Board. A better question is… When should an impaired physician report to the Board? �As a rule, it is always better for a physician to selfreport rather than to be reported.

To Report or Not To Report… Does an impaired physician have to report to the Board? �Yes, will likely eventually have to report to the Board. A better question is… When should an impaired physician report to the Board? �As a rule, it is always better for a physician to selfreport rather than to be reported. �It is usually favorable to have advocacy

Treatment for Impaired Physician �The function of a treatment plan is rehabilitative and not punitive.

Treatment for Impaired Physician �The function of a treatment plan is rehabilitative and not punitive. �Confidentiality and anonymity should be maintained for impaired physicians during and after treatment.

Treatment for Impaired Physician �The function of a treatment plan is rehabilitative and not punitive. �Confidentiality and anonymity should be maintained for impaired physicians during and after treatment. �Many states achieve this through state Physician Health Programs (PHP).

Treatment for Impaired Physician �The function of a treatment plan is rehabilitative and not punitive. �Confidentiality and anonymity should be maintained for impaired physicians during and after treatment. �Many states achieve this through state Physician Health Programs (PHP). �Physician Health Programs are not directly associated with state medical boards.

Professional Health Programs �Purpose: �To assist, guide, and advocate for participants, so they can attain and maintain overall wellness while safely practicing in their chosen profession. �A PHP addresses any physical, emotional, and/or behavioral problem that might interfere with their ability to live meaningful and satisfying professional and personal lives.

Professional Health Programs �Services: �Confidential screening and referral �Consultation and guidance �Support and monitoring �Accountability thru documentation of compliance �Substance use disorders, mental/behavioral health problems, disruptive behavior, stress related problems, boundary disorders, physical illness

Professional Health Programs �Confidentiality: �Confidentiality is one of the core commitments! �PHP’s can only release information with the explicit authorization of the participant.

Professional Health Programs �Confidentiality: �Confidentiality is one of the core commitments! �PHP’s can only release information with the explicit authorization of the participant. �Authority: �Most PHP’s have NO disciplinary role or authority. �PHP activities are solely related to advocacy, education, wellness, and support.

Thank You! Thank you for your time and attention. Questions? ? ?
- Slides: 75