A Study of Significant Event Analysis at Three


 A Unique feature is that this would be Canadian data")


 Diagram CAUSES Equipment Process EFFECT People SIGNIFICANT EVENT Materials Environment Management")


 Physician (resident) 13% Inter-professional")











 Involves the structured investigation of individual episodes which have been")



- Slides: 25
A Study of Significant Event Analysis at Three Academic Primary Care Sites: What Have We Learned? Collaborators Markham Family Medicine Teaching Unit: John Maxted & Sara Moshiri Toronto Western Hospital Family Medicine Teaching Unit: Trish Marr, Lesley Adcock & Sarah Fleming Women’s College Hospital Family Practice Health Centre: Nicole Bourgeois, Lisa Fernandes & Carol Kitai
A Shared Vision Markham, Women’s College and Toronto Western Family Medicine Teaching Units have independently been using the SEA process as part of their patient safety strategies We should combine data and analyze results , creating a framework that would represent a reliable evaluation of SEAs as a model to reduce patient harm and improve quality of care. The collaborative approach would produce a critical volume for evaluation and allow us to share a variety of perspectives from different settings
A Shared Vision (Ctd) A Unique feature is that this would be Canadian data based in primary care We would do this study with intent to disseminate the results through presentations and publication
Reminder: What is SEA? Pringle’s SEA definition: A process in which individual episodes are analyzed in a systematic and detailed way to ascertain what can be learned about the overall quality of care, and to indicate any changes that might lead to future improvements. A SEA provides a structured framework which can guide the team when discussing and investigating a chosen significant event (NHS)
SEA: 7 Steps 1. Awareness and prioritization of significant 2. 3. 4. 5. 6. 7. event Information gathering Facilitated team-based meeting Analysis of the significant event Agree, implement and monitor change Write it up Report, share and review
Ishikawa (Fishbone) Diagram CAUSES Equipment Process EFFECT People SIGNIFICANT EVENT Materials Environment Management
Progress In Improving Patient Safety Study of 30 SEAs allowing for: Reflection Improvement initiatives Dissemination of our learning
Key Study Findings and Reflections
Individuals Reporting Incidents 3% 20% Patient / caregiver Physician (faculty) Physician (resident) 13% Inter-professional HC providers Administrative staff 63%
Reporting compared to Involvement in Incidents 35 Number of Incidents 30 25 20 15 10 5 0 Patient / caregiver Physician (faculty) Aware of incident from Involved in incident 1 30 16 26 Physician (resident) 6 18 Inter-professional Administrative staff HC providers 6 0 21 6
SEA Components Completed 100% 98% 96% 94% 93% 92% 90% 88% 87% 86% What happened? Why did it happen? Tools used? Improvement defined?
System Improvement 100% 93% 87% 80% 70% 63% 60% 50% 37% 40% 30% 20% 10% 0% Implemented (at least one) Sustained Shared learning Likelihood of recurrence
No SEAs involved patients and/or caregivers
SEA Type of Incidents 80% 70% 63% 57% 60% 53% 50% 37% 40% 30% 20% 10% 7% 10% 0% Information transfers Medication Diagnosis Transitions of External Patient Inter & intra- Medico-legal management care (Int) Transitions of confidentiality professional requirements care (Ext) relations
Contributing Factors 100% 90% 80% 70% 66% 60% 52% 50% 38% 40% 34% 31% EMR technology dysfunction Lack of resident orientation 30% 20% 10% 0% Inadequate administrative processes Miscommunciation Insufficient provider knowledge or skills Lack of internal team coherence
Levels of Potential and Actual Harm from Incidents 41% 56% Potential Harm No Potential Harm
Levels of Potential and Actual Harm from Incidents Potential harm Harm Low 0% 21% Mild 17% 0% Moderate 17% 34% Severe 7% 3%
SEA Reflections What We Achieved – A Learning Collaborative! Collaborative 3 FMTUs – diverse cultures & organizations Team – formin’, stormin’, normin’ & performin’ Learning – Data Interpretation An orange is not an orange! An orange could be a lemon, a grapefruit, or maybe even an apple! Learning – Data Analysis What we expected What we didn’t expect Passion for SEA as a tool for PS awareness, engagement & improvement At least 4 other FMTUs engaged in PS through SEA
SEA Reflections What We Did Not Achieve – Too Ambitious? Enuf time to enjoy performin’ Study SEA impact on culture Commentaries 1. Medico-legal issues 2. Clash of cultures 3. Patient involvement 4. Safe language 5. Human vs system factor analysis Publication & Presentation*** Reflect Canadian experience in PS e. g. BMJ (+++), CFP, CMAJ, etc. Stay Tuned! SEA
Significant Event Analysis How SEAs Contribute to Safe, Reliable & Effective Care
Significant Event Analysis (SEA) Involves the structured investigation of individual episodes which have been identified by a member or members of the health care team as ‘significant’ SEA improves the quality and safety of patient care by encouraging reflective learning and, where necessary, the implementation of change to minimize recurrence of the events in question. Quality in Primary Care 2013; 21: 123– 30
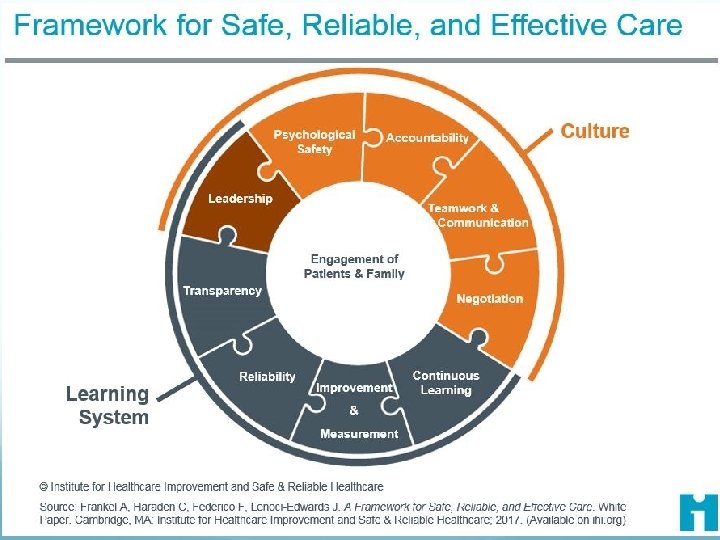
Significant Event Analysis IHI Framework For Safe, Reliable and Effective Health Care
SEA Reflections Comments & Questions?
References Kingston-Riechers J, Ospina M, Jonsson E, Childs P, Mc. Leod L, & Maxted J. (2010). Patient Safety in Primary Care. Edmonton, AB: Canadian Patient Safety Institute and BC Patient Safety & Quality Council Panesar SS, de. Silva D, Carson-Stevens A, et al. How Safe Is Primary Care: A Systematic Review. (2016) BMJ Qual Saf 25: 544– 553.