A review of PTOT in the ICU considerations













 • • Preexisting dementia History")
 • Changing")













- Slides: 34
A review of PT/OT in the ICU: considerations for early mobility programs By: Adam Miller
Overview • Background • The effects of immobility • The benefits of early mobilization • Barriers to mobility and strategies to overcome • Determining when PT/OT is appropriate • Criteria and Contraindications • Assessing Delirium & Sedation/Agitation • Early Mobilization programs • Phases • Summary
Objectives • Recognize the need for early therapy in the ICU • Identify barriers to mobility • Determine when therapy is appropriate for an ICU patient • Understand delirium and sedation and their impact in the ICU • Identify measures for assessing cognition and directing treatment • Describe a protocol and guidelines for implementing early mobility
Bed rest and immobility in the ICU 1, 3, 4, 7 • Immobility Effects • • • Deconditioning, muscle weakness, polyneuropathy, myopathy Atrophic processes begin within 72 h Skeletal muscle mass lost at a rate of 5% per week (other studies report as high as 20% per week) Weakened muscles generate increased oxygen demand, making ventilation weaning difficult Orthostatic Intolerance—A shift of intravascular fluid away from the extremities to the thoracic cavity caused by the removal of gravitational stress. • Mechanical Ventilation • Typically requires increased sedation • Following 18 hours of mechanical ventilation structural and functional changes occur in diaphragm • Combined with immobility—joint mobility restrictions, muscle weakness, critical illness neuromyopathies, pressure ulcers, DVT, prolonged ventilation, psychological disturbances • ICU long term effects • Functional disability and impaired quality of life up to 5 years after hospitalization • Memory and attention deficits, post-traumatic stress, depression, anxiety • ICU acquired weakness and neuromuscular weakness may not ever fully recover
Body Systems affected by Critical Illness • Nordon-Craft
The impact of early mobilization in the ICU 3, 4, 7 • Reduce and prevent complications • Increased weaning rates, time spent without a ventilator, and decreased duration of Mechanical Ventilation • Decrease in dyspnea and increase in peripheral muscular strength, respiratory muscle strength, functional capacity, and quality of life • Shorter duration of ICU-associated delirium • Associated with decreased ICU LOS and hospital LOS • Increased likelihood to d/c home and/or return to home sooner • Safe and well tolerated with both functional and psychological outcomes
Mobility Barriers & Keys to Overcoming 3, 8 • Safety • Physiological Instability • Clear guidelines • Daily screening and brief team discussion before each therapy session • Collaboration • Respiratory Therapists: present for all ventilated patients performing out of bed activity • Nurses: discuss medical status & POC, administer meds, assist as needed • Lack of a clear program • Leadership, knowledge, referrals • Interdisciplinary collaboration • Communicate and educate one another
Mobility Barriers & Keys to Overcoming 3, 8 • Sedation • Coordination with nurses to time therapy with sedation interruption/neuro checks • Time • Coordination of care >> Actual time to perform the activities • Staffing, training, equipment • Work with what ya got
Indications & Contraindications 4, 8 • When to start • When medically stable and able—the earlier the better • Studies vary— e. g. within 72 hours of MV, within 48 hours of start of critical care • Prioritize based on duration of bed rest & individuals requiring mechanical ventilation (especially greater than 3 days of mechanical ventilation)
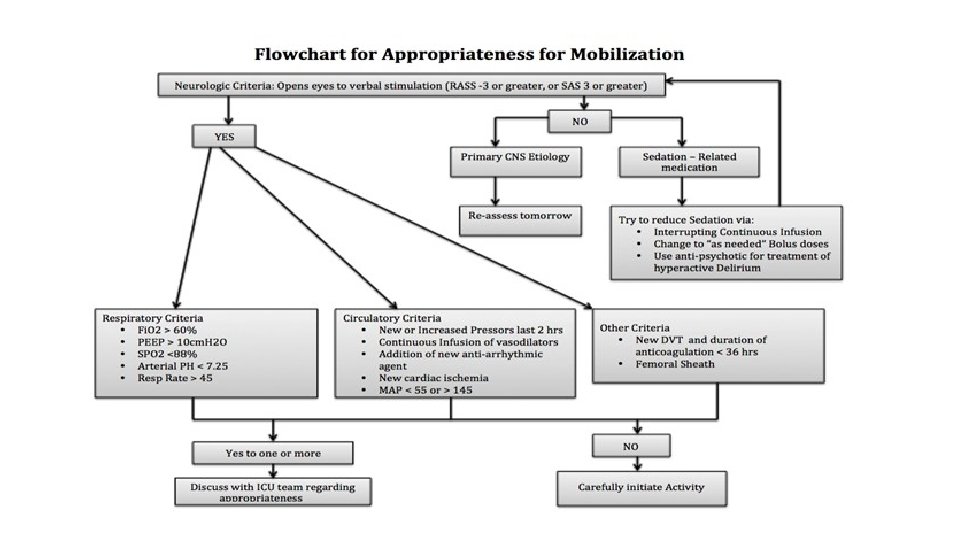
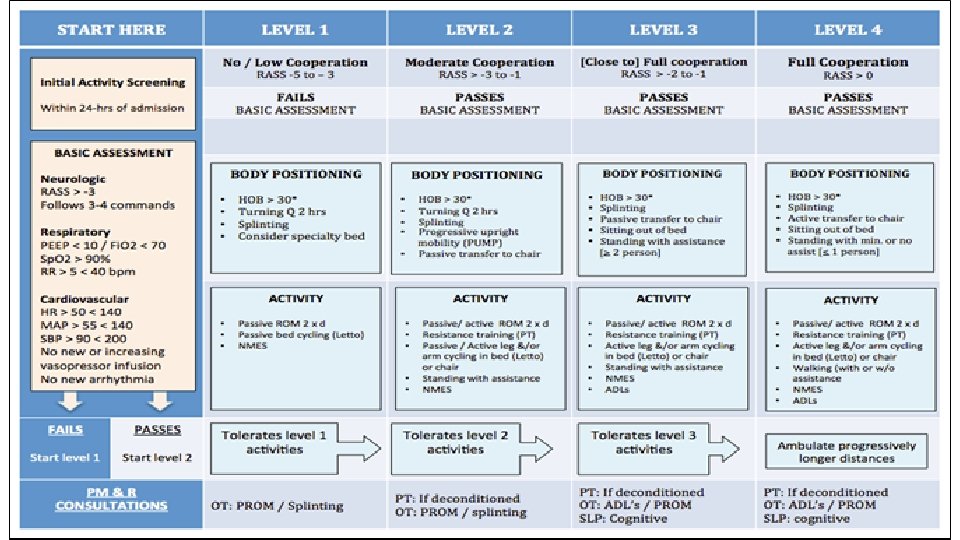
Indications & Contraindications 4, 8 • Medical Stability Criteria • • • Mean Arterial Blood Pressure between 65 – 110 mm Hg Systolic BP between 90 – 200 mm Hg HR between 40 – 130 bpm Respiratory rate between 5 – 40 breaths per min Sa. O 2 ≥ 88% Fi. O 2 less than 0. 6 • Evaluate each patient individually & monitor throughout session
Indications & Contraindications 3, 4, 8 • Contraindications • • • Elevated intracranial pressure Active GI blood loss Active myocardial ischemia Continuous procedures involving intermittent hemodialysis Pt agitation requiring increased sedative administration in past 30 minutes Unsecure airway Marked ventilator asynchrony Pt distressed or combative New arrhythmia Critical Hemodynamic Monitoring Concern for myocardial ischemia or airway device integrity
Other Factors affecting Patient Readiness • Cognition • Delirium • Sedation & Agitation
Delirium 4, 6 • A syndrome characterized by the acute onset of cerebral dysfunction with a change or fluctuation in baseline mental status, inattention, and either disorganized thinking or an altered level of consciousness • Hyperactive – agitation, emotional liability (less common) • Hypoactive – apathy, diminished responsiveness (more common) • Mixed • • • Affects up to 80% of mechanically ventilated adult ICU patients Costs $4 to $16 billion in the United States annually ICU delirium is an independent risk factor for numerous adverse outcomes Patients with delirium have decreased participation in mobility sessions Link between Delirium and neuromuscular function • Without intact cognition, physical activity is either self-limited or iatrogenically limited, cooperation with therapy is poor, and any immobilisation injury is likely to be exacerbated. Patients in post-acute care with persistent delirium have shown poor functional recovery
Delirium Risk Factors 2 • Baseline Risk Factors (non-modifiable) • • Preexisting dementia History of hypertension History of alcoholism High severity of illness at admission • Risk Factors (modifiable) • Immobility • Environmental • Pharmacological • Independent Risk Factor • Coma
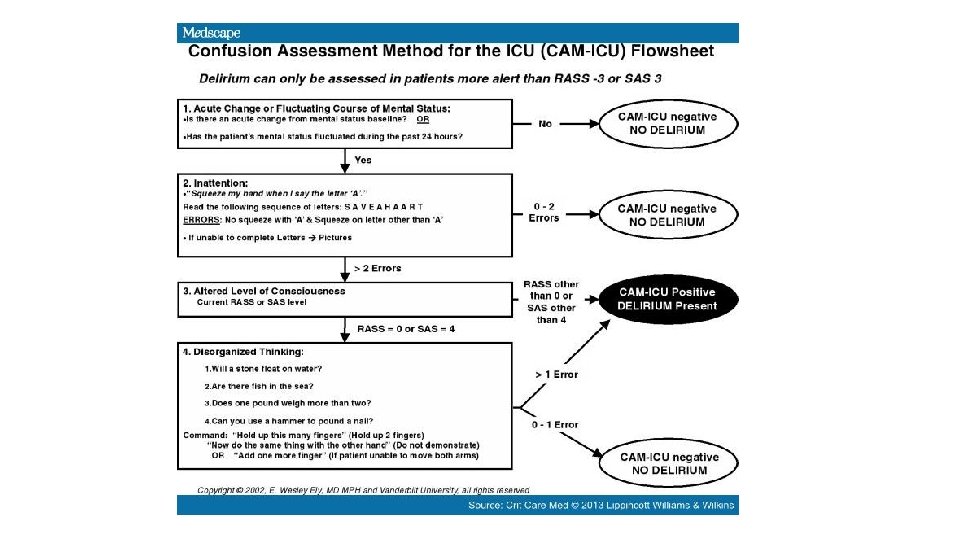
Assessing Delirium 2 • The Confusion Assessment Method for the ICU (CAM-ICU) • Changing mental status, inattention, altered level of consciousness, and disorganized thinking • The Intensive Care Delirium Screening Checklist (ICDSC) • An 8 checklist of delirium symptoms evaluated over an 8 - to 24 -hour period.
Tips for decreasing Delirium. Jen • Diurnal cycles • Light access during day, lights & T. V. off at night, wear glasses during day, take off at night • Routine • Meals • Activity—e. g. reading the paper, phone call, visit • Encourage journal keeping to keep track of therapy, doctor visits, etc. • Family pictures • Discuss with patient who they know in the picture/where it was taken • Mobility • OOB to chair or seated EOB at least 3 x/day
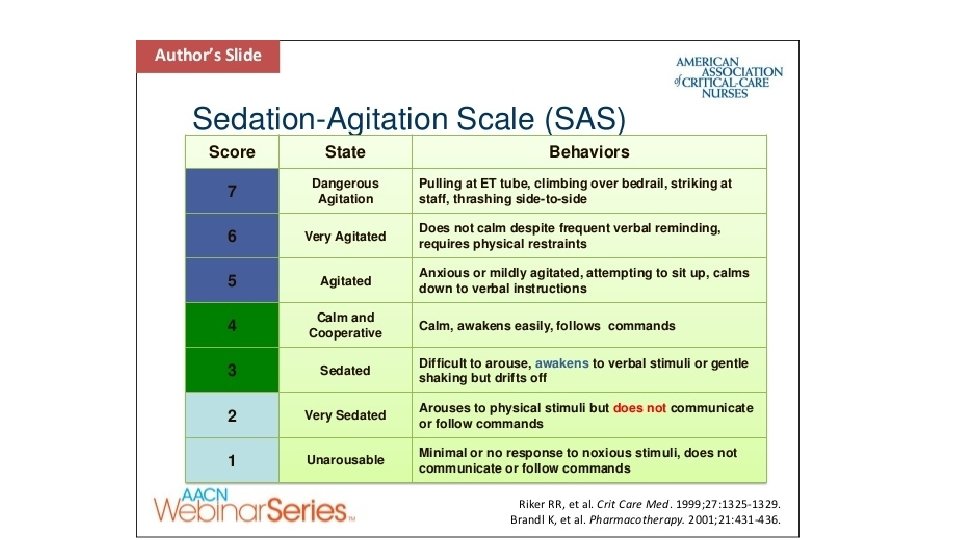
Sedation 2 • The Richmond Agitation and Sedation Scale • Sedation Agitation Scale
The Richmond Agitation and Sedation Scale • Score of >/= -3 is indication for non-pharmacological intervention
Early Mobilization Program Necessities 4, 8 • Effective intervention requires inter-professional collaboration • Physicians and physician assistants, nurses, respiratory therapists, physical therapists, occupational therapists • Daily determination/assessment of patient status • Sedation level • Delirium • Medical stability • Interruption of sedation, protocol driven spontaneous breathing trials, and timing with physical and occupational therapy • Result in better outcomes compared with standard approaches
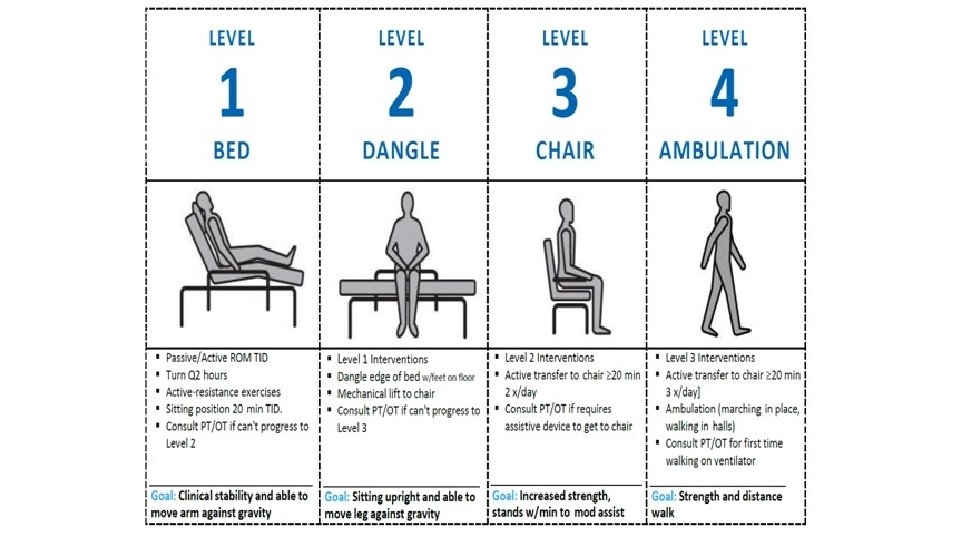
Early Mobilization Program: 4 Phases 8 Requirements: Able to follow commands, hemodynamic stability, acceptable oxygenation • Phase 1: Unstable and limited activity tolerance and/or inability to walk • Goal: sit at EOB unsupported or with minimal assistance and initiate standing activities • Progression criteria: stand with walker and tolerate full standing posture with weight shifts • Phase 2: Stable most of the time, continued limited activity tolerance • Goal: initiate transfer training with walker, initiate walking reeducation with walker • Progression criteria: transfer to chair with walker and assistance, tolerates walking re-education with walker • Phase 3: Multiple problems still present or resolving, able to participate actively in therapy • Goal: initiate independent transfer training with walker, provide progressive walking reeducation • Progression criteria: patient tolerates progressive walking program and increased activity levels • Phase 4: Pt weaned from mechanical ventilation, able to participate actively in therapy, working toward independence and d/c • Goal: promote progressive transfers and walking independence, promote independence with exercises and mobility program
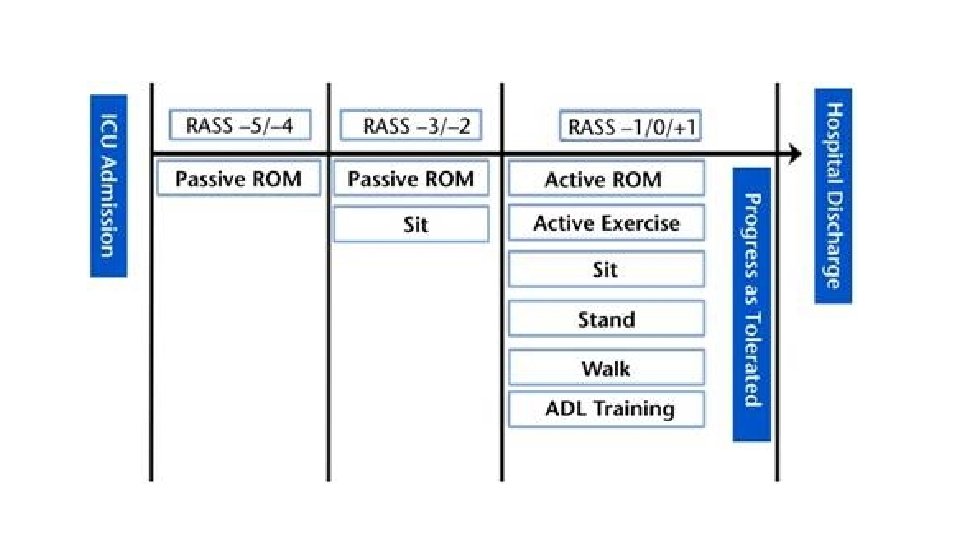
Early Mobilization Program—Phase 08 • Patients with insufficient level of arousal/contraindications to activity • Standard nursing care including positioning every 2 hours and PROM • PROM has been shown to enhance ventilation in neurological patients in highdependency units • Skilled PROM done by PT—patients with burns • Daily PT/OT screening
Early Mobilization Program—Phase 18 Duration & Frequency: 15 -30 minutes as tolerated, once daily, 1 -7 days/week Education Intervention Positioning Bed mobility Training Transfer training Walking Program Exercises Phase 1 Instruction of patient and patient’s family members on the importance of positioning, exercise program, and early mobility Focus on preventing pressure ulcers, especially on heels and sacrum Recommendations for appropriate program for patients with orthopedic and/or neurological deficits Turning side to side Scooting/bridging Supine ↔ sitting Sitting on side of bed associated with • leg exercises • breathing exercises • balance/coordination exercises for trunk control • self-care activities • unsupported sitting Transfer out of bed only to stretcher chair with total assistance Initiation of sit to stand with walker and assistance as appropriate Patients not ambulatory Focus on attempts to stand with walker and prewalking activities Inclusion of one or a combination of • passive range of motion • active assisted range of motion • active range of motion • stretching • resistance exercise on leg press, light weights (1 -5 lb [0. 45 -2. 25 kg]), and/or exercise band • breathing exercises (deep breathing, coughing, incentive spirometer)
Early Mobilization Program—Phase 28 Duration & Frequency: 15 -45 minutes as tolerated, once daily, 5 -7 days/week Intervention Education Phase 2 Same as phase 1, plus instructions on • proper use of walker • safety during transfers • importance of gradual increase in time sitting out of bed Positioning Same as phase 1 Bed mobility Training Same as phase 1 Transfer training Transfers training to using walker and assistance to • bedside chair • bedside commode • stretcher chair (to facilitate safe transfers back to bed) Walking Program Initiation of walking reeducation with walker and assistance Exercises Same as phase 1
Early Mobilization Program—Phase 38 Duration & Frequency: 30 -60 minutes as tolerated, once daily, 5 -7 days/week Education Intervention Positioning Bed mobility Training Transfer training Walking Program Exercises Phase 3 Same as phase 2, plus instructions on • importance of progressive mobilization • safety issues during transfers and walking Not a concern if patients tolerate several hours out of bed, unless orthopedic and/or neurological deficits still present Gradual withdrawal of assistance Initiation of training to promote patient’s independence Gradual withdrawal of assistance during transfers to chair and bedside commode with nursing staff and/or family assistance Walking reeducation with focus on gradual increase in distance and endurance Gradual withdrawal of assistive device if appropriate Same as phase 1
Early Mobilization Program—Phase 48 Duration & Frequency: 30 -60 minutes as tolerated, once daily, 5 -7 days/week Education Intervention Positioning Bed mobility Training Transfer training Walking Program Exercises Phase 4 Discharge planning Family training on bed mobility, transfers, and walking Safety issues during transfers and walking Home exercise and activity program with guidelines for progression and selfmonitoring Not a concern unless orthopedic and/or neurological deficits still present Focus on training to promote independence Family training on selected issues as appropriate Promotion of independence during transfers with or without assistive device Family training if appropriate Gradual withdrawal of assistive device if appropriate Gait reeducation on different surfaces as needed, including stairs, curb, ramp, carpet (some patients may benefit from wheelchair mobility training if still unable to walk) More intense strengthening and endurance exercises as appropriate, including • arm ergometry • treadmill • stationary bike • leg press • stairs training • inspiratory muscle training
Summary • Early mobility in the ICU is a challenge, but is worth the effort to implement a coordinated program • Interdisciplinary teamwork is crucial • There available criteria for determining patient readiness for therapy that have been shown to be safe and effective • Patient stability, cognition, and level of arousal must be assessed and discussed with the team before proceeding with any session • Early mobilization guidelines exist to help guide progression of intervention strategies and facilitate positive patient outcomes
References 1. Banerjee A, Girard TD, Pandharipande P. The Complex Interplay between Delirium, Sedation, and Early Mobility during Critical Illness: Applications in the Trauma Unit. Current opinion in anaesthesiology. 2011; 24(2): 195 -201. doi: 10. 1097/ACO. 0 b 013 e 3283445382. 2. Barr J, Fraser G, Skrobik Y, et al. Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Best Practices For Hospital & Health-System Pharmacy [serial online]. January 2014; : 684 -730. Available from: CINAHL Plus with Full Text, Ipswich, MA. Accessed May 1, 2017. 3. Clark DE, Lowman JD, Griffin RL, Matthews HM, Reiff DA. Effectiveness of an Early Mobilization Protocol in a Trauma and Burns Intensive Care Unit: A Retrospective Cohort Study. Physical Therapy. 2013; 93(2): 186 -196. doi: 10. 2522/ptj. 20110417. 4. Early physical and occupational therapy in mechanically ventilated, critically ill patients: a randomised controlled trial. The Lancet [serial online]. 2009; (9678): 1874. Available from: General Reference Center Gold, Ipswich, MA. Accessed May 1, 2017. 5. Gosselink R, Bott J, Johnson M, et al. Physiotherapy for adult patients with critical illness: recommendations of the European Respiratory Society and European Society of Intensive Care Medicine Task Force on Physiotherapy for Critically Ill Patients. Intensive Care Medicine. 2008; 34(7): 1188 -1199. doi: 10. 1007/s 00134 -008 -1026 -7. 6. Kamdar B, Combs M, Colantuoni E et al. The association of sleep quality, delirium, and sedation status with daily participation in physical therapy in the ICU. Critical Care. 2016; 20(1). doi: 10. 1186/s 13054 -016 -1433 -z. 7. Laurent H, Aubreton S, Coudeyre E, et al. Review: Systematic review of early exercise in intensive care: A qualitative approach. Anaesthesia Critical Care & Pain Medicine [serial online]. April 1, 2016; 35: 133 -149. Available from: Science. Direct, Ipswich, MA. Accessed May 1, 2017. 8. Perme C, Chandrashekar R. Early Mobility and Walking Program for Patients in Intensive Care Units: Creating a Standard of Care. American Journal Of Critical Care - An Official Publication, American Association Of Critical-Care Nurses [serial online]. 2009; (3): 212. Available from: Oa. Findr, Ipswich, MA. Accessed May 1, 2017. 9. 4 E’s for Early Mobility Pat Posa RN, BSN, MSA, FAAN System Performance Improvement Leader St. Joseph Mercy Hospital Ann Arbor MI 10. Campbell M, Fisher J, Anderson L, Kreppel E. Implementation of Early Exercise and Progressive Mobility: Steps to Success. Critical Care Nurse [serial online]. February 2015; 35(1): 82 -88. Available from: CINAHL Plus with Full Text, Ipswich, MA. Accessed May 2, 2017.
Questions? Comments? Compliments?