A reduced dose of iodinated contrast medium can

 • Good quality negative CT pulmonary angiogram (CTPA) can reliably exclude the")

 • Significance – Majority clinically silent, resolves 1 -2 weeks •")

 • Aim: achieve maximum contrast opacification of pulmonary arteries using minimum dose")
 • George Eliot Hospital NHS Trust • 2 methods performing CTPA –")
 antecubital fossa")
 • Bolus tracked on main pulmonary artery. • Scan started manually when")


 • The groups did not differ significantly in terms of age (p=0.")
 Group Mean dose (g/ Iodine) Opacification Pulmonary Trunk (HU) Suboptimal Studies (<250")
 Attenuation (HU)")
 • Mean dose of contrast is 12% lower in the 75 ml")








 were analysed using the")





![• In a different single cohort study [9], the authors have evaluated the](https://slidetodoc.com/presentation_image_h/e0547972ea23a8772a1d737c79db0ec8/image-31.jpg "• In a different single cohort study [9], the authors have evaluated the")
 but")








![References • • [1] National Institute for Health and Care Excellence. Venous thromboembolic diseases:](https://slidetodoc.com/presentation_image_h/e0547972ea23a8772a1d737c79db0ec8/image-41.jpg "References • • [1] National Institute for Health and Care Excellence. Venous thromboembolic diseases:")
![• • [7] Goble EW and Abdukarim JA, CT pulmonary angiography using a](https://slidetodoc.com/presentation_image_h/e0547972ea23a8772a1d737c79db0ec8/image-42.jpg "• • [7] Goble EW and Abdukarim JA, CT pulmonary angiography using a")
- Slides: 42
A reduced dose of iodinated contrast medium can be used in CT pulmonary angiography without adversely affecting image quality Dr J Abdulkarim FRCSEd, FRCR Consultant Radiologist George Eliot Hospital NHS Trust
Background (1) • Good quality negative CT pulmonary angiogram (CTPA) can reliably exclude the presence of pulmonary emboli 1 – Important aspect of quality is degree of opacification of the pulmonary arteries – Degree of arterial enhancement depends upon intravascular iodine concentration of target vessel at time of scanning 2 • BUT risk of contrast induced nephrotoxicity is related to dose 3 1. 2. British Thoracic Society guidelines for the management of suspected acute pulmonary embolism. Thorax 2003; 58: 470 -484 Fujikawa A, Tsuchiya K, Imai M, Nitatori T. CT angiography covering both cervical and cerebral arteries using high iodine concentration contrast material with dose reduction on a 16 multidetector- row system
Contrast induced nephropathy • • • Acute decline in renal function after administration of an iodinated contrast agent in the absence of an alternative cause 3 Rise in serum creatinine >25% or 44 micromol/l from baseline 4, 5 Incidence (using above definition) 0. 6 - 2. 3% overall 6 Up to 16. 8% in high risk patients 7 Chronic kidney disease (Cr. Cl < 60 ml/min) is most important risk factor for developing CIN 3, 4 3. Morcos SK, Thomsen HS, Webb JAW and members of the Contrast Media Safety Committee of the European Society of Urogenital Radiology (ESUR). Euro. Radiol 1999; 9: 1602 -1613 4. Thomsen H. Guidelines for contrast media from the European Society of Urogenital Radiology. AJR 81; 1463 -1471, 2003. 5. Mc. Cullough P, Sandberg KA. Epidemiology of contrast induced nephropathy. Rev Cardiovasc Med 4 (Suppl 5): S 3 -S 9, 2003. 6. Lasser E, Lyon SG, Barry CC. Report on contrast media reactions: Analysis of data from reports to the US Food and Drug Administration. Radiology 203: 605 -610, 1997. 7. Solomon R. The role of osmolality in the incidence of contrast- induced nephropathy: A systematic review of angiographic contrast media in high risk patients.
Contrast induced nephropathy(2) • Significance – Majority clinically silent, resolves 1 -2 weeks • Increased incidence non- renal complications – Sepsis, bleeding, stroke, respiratory failure – Prolonged hospital stay and increased morbidity/ mortality – Those who develop CIN are at higher risk of death in hospital and at 1 year 8 8. Mc. Cullough P, Wolyn R, Rocher LL, et al. Acute renal failure after coronary intervention: Incidence, risk factors, and relationship to mortality. Am J Med 103: 368 - 375, 1997.
Contrast induced nephrotoxicity • Risk factors – Renal impairment – Dehydration – Congestive cardiac failure – Over 70 years of age – Nephrotoxic drugs
Background (2) • Aim: achieve maximum contrast opacification of pulmonary arteries using minimum dose of contrast medium 3 3. Morcos SK, Thomsen HS, Webb JAW and members of the Contrast Media Safety Committee of the European Society of Urogenital Radiology (ESUR). Euro. Radiol 1999; 9: 1602 -1613
Background (3) • George Eliot Hospital NHS Trust • 2 methods performing CTPA – 100 ml i. v. Optiray 300 (300 mg I/ml) = 30 g I – 75 ml i. v. Optiray 350 (350 mg I/ml) = 26. 25 g I – Introduced October 2010 - manufacturer recommendation • Both licensed in UK • Potential benefits – Reducing iodine load (and risk of nephrotoxicity) – Reducing cost
Technique • GE lightspeed 32 slice scanner. • 18 g cannula (Green) antecubital fossa • 100 ml group – 5 ml/s (20 seconds) • 75 ml group “Optibolus” function – 5 ml/s – decreases exponentially during injection to 4. 2 ml/s (16 seconds)
Technique (2) • Bolus tracked on main pulmonary artery. • Scan started manually when 100 HU in main pulmonary artery.
Aim • To investigate if there is a difference in diagnostic quality of CTPAs obtained using the two techniques based on degree of opacification of the pulmonary arteries
Methodology • CTPA images reviewed retrospectively – 69 patients who received 100 ml 300 mg I/ml – 70 patients who received 75 ml 350 mg I/ml • Contrast opacification measured in main pulmonary artery • Considered suboptimal if opacification <250 HU 4 • Patient demographic data collected from notes – Sex, age and weight. 4. Ramadan SU, Kosar P, Sonmez I et al. Optimisation of contrast medium volume and injection- related factors in CT pulmonary angiography: 64 - slice CT study. Euro. Radiol 2010; 20: 2100 -2107 5. Bae KT, Tao C, Gurel S et al. Effect of patient weight and scanning duration on contrast enhancement during pulmonary multidetector CT angiography. Radiology 2007; 242 (2): 582 -589.
Results (1) • The groups did not differ significantly in terms of age (p=0. 263), sex (p=0. 396) or weight (p=0. 169)
Results (2) Group Mean dose (g/ Iodine) Opacification Pulmonary Trunk (HU) Suboptimal Studies (<250 HU Pulmonary Trunk) 100 ml 300 mg I/ml 29. 53 (sd = 0. 587) (95% CI 29. 3829. 67) 331. 39 (sd = 82. 62) (95% CI 311. 5351. 2) 13 (18%) 75 ml 350 mg I/ml 26. 25 (sd = 0) (95% CI 26. 25) 365 (sd = 118. 38) (95% CI 336. 7393. 3) 12 (17%) p value p < 0. 0001 p = 0. 0546 p = 0. 83
Results (3) Attenuation (HU)
Results (3) • Mean dose of contrast is 12% lower in the 75 ml 350 mg I/ml group • But mean opacification of the pulmonary trunk is greater in 75 ml 350 mg I/ml (did not quite meet statistical significance) • No significant difference in number of suboptimal studies
Limitations • Retrospective data collection • Higher opacification in 75 ml 350 mg I/ml group not statistically significant – BUT was equal • Contrast opacification is only one aspect of quality • Study has shown potential rather than actual patient safety benefits
• Goble EW and Abdukarim JA, CT pulmonary angiography using a reduced volume of highconcentration iodinated contrast medium and multiphasic injection to achieve dose reduction, Clinical Radiology 2014; 36 -40.
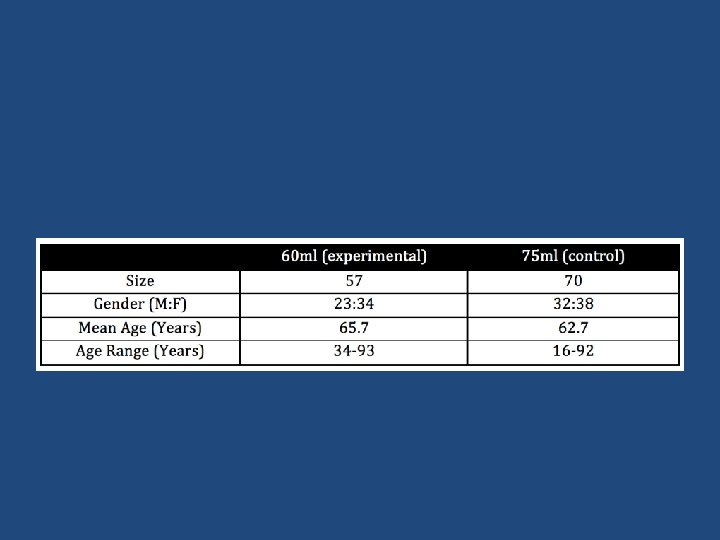
2015 Second study Methods and materials : • 127 patients clinically suspected of having pulmonary embolism underwent spiral CTPA; one group received 75 ml and the other a reduced dose of 60 ml of 350 mg iodine/ml Ioversol (Omnipaque 350, GE Healthcare). Both patient cohorts were studied retrospectively.
CTPA protocol • Scans were performed using a 128 slice CT system (Somatom, Siemens Healthcare, Erlangen, Germany). • Acquisition parameters 120 k. Vp, automatic m. A (dose modulated), 800 m. A maximum tube current, 0. 6 s rotation time, pitch factor 1. 375: 1, noise index 28, 1. 25 mm slice thickness with 40 mm beam collimation.
• 18 G cannula in the ante-cubital fossa. • Contrast delivered via a power injector at an initial rate of 5 ml/s then decreasing exponentially to 4. 2 ml/s over the duration of the injection using bolus shaping software, resulting in a total injection time of 16 seconds. • A 25 ml saline chaser was given, at the same rate.
• Initiation of the scan using a bolus tracking method, placing a region of interest (ROI) in the main pulmonary artery. • The initial low-dose monitoring image at 3 s and was repeated every 2 seconds. • The scan was triggered manually when the threshold of 100 HU was reached in the main pulmonary artery. Then a delay of 5. 5 seconds ensued, for the scan table to move from the monitoring position to the start position during which time the patients were asked to halt their breathing. • CTPAs were obtained in a craniocaudal direction with images obtained from the lung apices to the diaphragm.
• Demographic data including patient age and sex were either recorded at time of scanning or obtained retrospectively from the patients’ hospital records. Patient weight was not examined in this study.
Image Assessment : • Image assessment was performed retrospectively by a single clinician on insignia picture achieving and communication system (PACS) workstation. • Image opacification was measured in the main, right and left pulmonary arteries. • There is no agreed threshold for minimal contrast opacification but 250 HU is used widely in various literature [6], and was thus adopted in our study.
Statistical Analysis: • Categorical variables (gender, number of rejected scans) were analysed using the chi-square test. The correlation between weight and age with opacification was analysed with Pearson’s correlation coefficient. General linear model analysis of variance (GLM) was performed to investigate the association between demographic variables and difference in attenuation. All statistical tests were conducted at a significance level of p < 0. 05. Statistical analyses were performed using Microsoft Excel 2010 (Microsoft Corp, USA).
Results
Results: • There was no significant difference between the groups in either age (p = 0. 35) or sex (p = 0. 42). • The mean opacification in the main, right and left pulmonary arteries are given in Table 2. Note that although the values are higher with 75 ml of contrast medium, the difference is not significant enough to affect the overall image quality
• Mean opacification was found to be positively correlated to patient age (Pearson’s correlation 0. 426, p < 0. 0001). When age is accounted for, the two groups did not differ significantly in terms of their mean opacification in the main (437 vs 438, p = 0. 48), left (417 vs 420, p = 0. 45) or the right pulmonary arteries (417 vs 424, p = 0. 40). • Taking an acceptance threshold of 250 HU, the rate of rejected scans did not differ significantly between the two groups, as shown in Table 3.
Discussion • Various past literature have assessed the use of a lower dose contrast medium in CTPA. In one study [7], the feasibility of using a reduced dose of contrast material (75 ml) delivered in a higher concentration (350 mg iodine/ml Ioversol) compared to the conventional 100 ml of 300 mg iodine/ml Ioversol was assessed and successfully established. This finding was also reported in a Randomised Clinical Trial published in the same year , which further established the use of a lower energy tube (80 k. Vp vs 100 k. Vp) for a reduced dose of radiation. In a different single cohort study [9], the authors have evaluated the practicality of CTPA with 30 ml of contrast medium in patients with renal impairment. Although it was stated that only one out of 24 scans were non-diagnostic, the reported average opacification (247 HU) in the main pulmonary arteries is notably lower than that found in our study and is below the 250 HU threshold that we have used. Furthermore, this work did not include a control group thus provided weaker evidence than the case control studies.
• In a different single cohort study [9], the authors have evaluated the practicality of CTPA with 30 ml of contrast medium in patients with renal impairment. Although it was stated that only one out of 24 scans were non-diagnostic, the reported average opacification (247 HU) in the main pulmonary arteries is notably lower than that found in our study and is below the 250 HU threshold that we have used. Furthermore, this work did not include a control group thus provided weaker evidence than the case control studies.
• The risk of CI-AKI is low in the general population (<2%) but can be as high as 10 -40% in patient with certain risk factors (diabetes, cardiac failure, pre-existing renal impairment, older age and recent exposure to nephrotoxic drugs). However, these patients are equally, if not more, likely to be at a risk of developing PE. • Since the risk of CI-AKI is known to be dose-dependent , it is desirable to use as small an amount of contrast medium as possible. • Additionally, the propsoed reduction in contrast medium dose can lower the cost by about 15% per scan.
• For determining the number of suboptimally opacified scans, we have adopted an acceptance threshold of 250 HU. It is important to note that there is no overall consensus on this cutoff and various figures (200 HU, 250 HU, 300 HU) have been quoted in past literature [11, 12]. The threshold of 250 HU was chosen based on the authors’ own clinical experience, that a single radiodensity measurement in the main pulmonary artery is often recorded when reporting on CTPAs and as such, an embolus can not be confidently ruled out if the minimum opacification was less than 250 HU.
• With this figure, the experiemntal and control groups have yielded a scan acceptance rate of 89% and 86%, respectively. This is comparable to the 88. 9% acceptance rate quoted in a study by Nazaroglu et al. , where a much higher contrast medium dose (100 ml of 350370 mg iodine/ml) was used.
Limitations: • A number of patient factors have been shown to affect the degree of vascular opacification. Mody notably, age has been demonstrated to have a positive correlation with the degree of opacification , which is reflected in our results. • Body weight another factor with a negative impact on image opacification , this was not assessed given the retrospective nature of our study and inconsistency of information availability amongst our patients. This remains a key limitation that needs to be better accounted for in future work.
• A third limitation is that the clinical observer making the opacification measurements was not blinded to the contrast dose used. However, since our analysis was purely restricted to objective observation, no subjective scoring was involved so this would be acceptable.
• Finally, we have focused our measurements on the central pulmonary vasculature whereas pulmonary embolus can also be found in the peripheries. • The isolation and sampling of smaller peripheral vessel can be technically difficult and potentially inaccurate, and it is therefore impractical to incorporate peripheral vessel measurements at this stage.
Latest work Working with Siemens UK: Further manipulation of scanning parameters: Scan delay reduced to 4 instead of 6 sec. The scan is triggered at 80 HU instead of 100. Kev is reduced to at least 100 (automated and can drop to 80 in slim patients). • Contrast volume is reduced to 45 ml. • • •
Results so far • 18 low dose CTPA. • All diagnostic studies with no suboptimal studies. • Lowest mean HU was 251 and highest 1152 • Radiation dose received by patient is reduced by 30 - 50% in all cases
Conclusion • Use of a reduced dose of high iodine contrast medium provides an equal degree of pulmonary arterial enhancement for CT pulmonary angiography • This has patient safety and cost implications • Current work with lower dose and adjustment of scanning parameters is providing very promising, and it times probably superior results at lower dose.
References • • [1] National Institute for Health and Care Excellence. Venous thromboembolic diseases: the management of venous thromboembolic diseases and the role of thrombophilia testing, CG 144. London: National Institute for Health and Care Excellence; 2012. [2] Fleischmann D. How to design injection protocols for multiple detector- row CT angiography (MDCTA). Eur Radiol Suppl 2005; 15(Suppl. 5): E 60 e 5. [3] Thomsen HS, Morcos SK, Barrett JB. Contrast-induced nephropathy: the wheel has turned 360 degrees. Acta Radiol 2008; 49: 646 e 57. [4] Lewington A, Mac. Tier R, Hoefield R, et al. Prevention of contrast induced acute kidney injury (CI-AKI) in adult patients. Royal College of Radiologist guidelines 2013. Available at: www. rcr. ac. uk/ [accessed 11. 12. 15]. [5] Bae KT, Tao C, Gurel S, et al. Effect of patient weight and scanning duration on contrast enhancement during pulmonary multidetector CT angiography. Radiology 2007; 242: 582 e 9. [6] Ramadan SU, Kosar P, Sonmez I, et al. Optimisation of contrast medium volume and injection-related factors in CT pulmonary angiography: 64 - slice CT study. Eur Radiol 2010; 20: 2100 e 7. [7] Goble EW and Abdukarim JA, CT pulmonary angiography using a reduced volume of high-concentration iodinated contrast medium and multiphasic injection to achieve dose reduction, Clinical Radiology 2014; 36 -40.
• • [7] Goble EW and Abdukarim JA, CT pulmonary angiography using a reduced volume of high-concentration iodinated contrast medium and multiphasic injection to achieve dose reduction, Clinical Radiology 2014; 36 -40. [8] Szusc-Farkas Z, Christe A, Megyeri B et al. Diagnostic accuracy of computed tomography pulmonary angiography with reduced radiation and contrast material dose: a prospective randomized clinical trial, Invest Radiol 2014; 201 -8. [9] Singh T, Lam KV and Murray C. Low volume contrast CTPA in patients with renal dysfunction, J Med Imaging Radiat Oncol, 2011; 1754 -9485. [10] Tsuchiya K, Honya K, Yoshida M, Gomyo M, Nitatori T. Cerebral CT angiography using a reduced dose of contrast material at high iodine concentration in combination with a saline flush. Clin Radiol 2008; 63: 1332 e 5. [11] Roggenland D, Peters SA, Lemberg SP, et al. CT angiography in suspected pulmonary embolism: impact of patient characteristics and different venous lines on vessel enhancement and image quality. Am J Roentgenol 2008; 190: W 351 e 9. [12] Bae KT, Tao C, Gurel S, et al. Effect of patient weight and scanning duration on contrast enhancement during pulmonary multidetector CT angiography. Radiology 2007; 242: 582 e 9. [13] Nazaroglu H, Ozmen CA, Akay HO, et al. 64 -MDCT pulmonary angiography and CT venography in the diagnosis of thromboembolic disease. Am J Roentgenol 2009; 192: 654 e 61. [14] Lee CH, Goo JM, Lee HJ, et al. Determination of optimal timing window for pulmonary artery MDCT angiography. Am J Roentgenol 2007; 188: 313 e 7.