A Practical Approach to Paediatric ECG Interpretation on


 Is")














- Slides: 18
A Practical Approach to Paediatric ECG Interpretation on Dr J Cyriac Consultant Paediatrician
P wave • Atrial Contraction • Indication of atrial morphology • Does the p wave have a normal axis? (P waves are positive in I, II and a. VF) • Rt atrial enlargement: Peak P wave >2. 5 mm in II, V 1, V 2 • Lt atrial enlargement: P wave broad/bifid (P wave 0. 04 to 0. 08 in infancy. 0. 06 to 0. 1 sec in older children)
QRS complex • • Ventricular depolarisation Duration: 0. 06 to 0. 08 sec) Is the net QRS voltage in lead a. VF positive Is the net QRS voltage in the lead I negative (normal neonate) or positive (normal child) Normal QRS Axis Newborn: +135(+60 to +180) At one year +60(+60 to +100) At 14 years: +60
QRS complex/Voltages • • Q wave: Septal depolarisation Normal in lead II, III, a. VF, V 5, V 6 Normal Q wave 2 to 3 mm QRS Voltage RV 1: Newborn 14 mm to 14 year 4 mm SV 1: Newborn 8 mm to 14 year 11 mm RV 6: Newborn 4 mm to 14 year 14 mm SV 6: Newborn 3 mm to 1 mm
QT interval and T wave • QT interval corrected to ventricular rate • QTc=QT interval divided by square root ot RR interval: Upper limit 0. 44 sec) • T wave: Ventricular repolarisation
RVH • Monophasic or pure R wave in V 1 V 4 R • Upright T wave in V 1 after 7 days until 7 years • R/S ration in V 1 : 0 -3/12: 6. 5, 3 -6/12: 4, 6/12 to 3 years: 2. 4 3 -5 years: 1. 6 • R in V 1 >20 mm at all ages • S wave in V 6 >15 mm in first week, 10 mm up to 6 months, 7 mm from 6 to 12 months, 5 mm above 1 year • T wave inversion extending to V 4 • Widening of QRS complex>0. 08
LVH • Tall R waves in V 5/V 6( >40 mm over 1 year, >30 mm under 1 year) • Deep S wave in V 1 • Q wave ≥ 4 mm in V 5/V 6 • Widening of QRS duration/Flattening of T waves in V 5, V 6 • T wave inversion in V 5, V 6 (Severe) • ST segment depression (Severe)
Biventricular Hypertrophy • Tall R waves and deep S waves in V 3, V 4 • R+S over 50 mm any age
Ostium Primum ASD
WPW Syndrome
TOF, TR, PR
Left Bundle Branch Block
Partial AVSD
Fallot’s Tetralogy
WPW syndrome
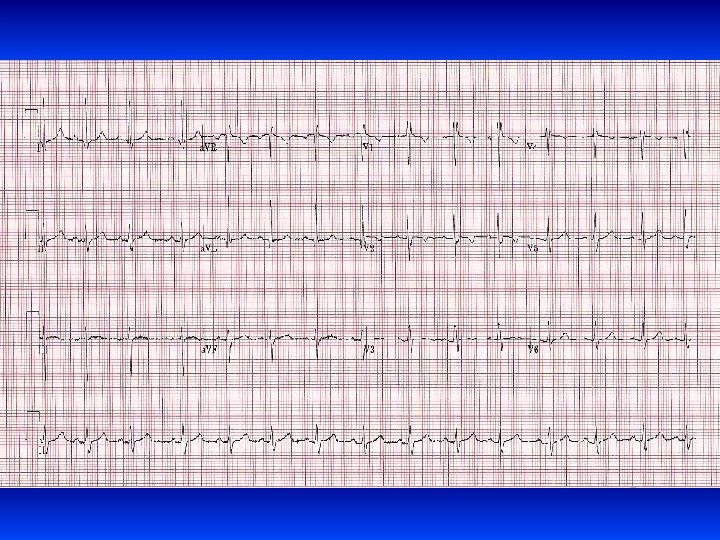
SVT
Summary • ECG in children is dynamic • All parameters of ECG varies as the baby grows into an adult • Don’t glance at ECG and come to a conclusion • Systematic examination of ECG is crucial • All paediatric trainees should have a paediatric ECG manual or App in hand!!