A New Group Treatment Approach towards Sex Offenders



 in the media https: //www. youtube. com/watch? v=i 5 jc.")


 O Excess axons in specific areas of the")














 O School-age (ages 4")























. Diagnostic and statistical manual of mental disorders (5 th")


- Slides: 52
A New Group Treatment Approach towards Sex Offenders on the Autism Spectrum Harmony Goorley MA, LCPC Harmony. Goorley@illinois. gov Jennifer Block, Psy. D. , LCP Marisa Quinones, Psy. D.
Agenda O O O O What is Autism Spectrum Disorder? How does ASD impact the client? Common difficulties associated with ASD Rationale for autism-specific treatment programming Structure of autism-specific programming Client experiences before and after program implementation Tips for treatment providers when interacting with individuals on spectrum Future Direction
IL Civil Commitment Facility O Secured residential facility for sexually violent adult males O Provide sex offense-specific treatment O Five stage treatment program using group therapy through all stages O Groups capped at 12 participants with 2 facilitators O Three to six 1. 5 hour group sessions each week O Committed - 369 O Detained - 191 O Total - 560 O Conditional Release - 45 (supervised in the community)
Autism Spectrum Disorder (ASD) in the media https: //www. youtube. com/watch? v=i 5 jc. L 2 D 3 F-8
Autism Spectrum Disorder Criteria A. Persistent deficits in social communication and social interaction O Deficits in social-emotional reciprocity O Deficits in nonverbal communicative behaviors used for social interaction O Deficits in developing, maintaining, and understanding relationships Criteria B. Restricted, repetitive patterns of behavior, interests, or activities O Stereotyped or repetitive motor movements, use of objects, or speech O Insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior O Highly restricted, fixated interests that are abnormal in intensity or focus O Hyper- or hypo-activity to sensory input or unusual interest in sensor aspects of the environment (American Psychiatric Association, 2013)
ASD and the brain O Delay in brain development as early as 6 months old O Blunted development of white matter that forms major information pathways between different brain regions O Excess brain cells/neurons or connections that impede functioning O In short, abnormal functional activity and organization affect different structures in different ways (Torun, Guney, Iseri, 2015)
Underconnectivity Theory (Shriber, L. , 2010) O Excess axons in specific areas of the brain cause over- connection, while the overall connection to other areas is weak O Lack of coordination between brain regions impacts integration of all information to aid in function
Neurotypical Social Cognition Gaus, 2011 INPUT The brain collects information from the environment, speech of others, and non-verbal cues of others (body posture, facial expressions) PROCESSIN G The brain processes the information and makes a decision to respond by placing meaning on others’ behaviors and the environment. OUTPUT The brain responds based on judgment by doing or saying something.
Social Cognition and ASD Gaus, 2011 INPUT Difficulty noticing social cues/reading other people • Overlooking or misinterpreting body language, posture, speech, and facial expressions • PROCESSIN G • Difficulty analyzing information to predict what a person is thinking, feeling, expecting, or planning (i. e. being aware of others’ perspectives) OUTPUT • Speak without considerin g others reactions
Social Skill Difficulties O Decreased ability to maintain relationships O Difficulty participating in new environments O Difficulty expressing empathy O At risk of isolation, rejection, and bullying
Communication: Base of Human Interaction O Process of sharing ideas, feelings, needs, desires O Powerful tool, weapon, manipulative agent… O Primitive beings used communication to gain control over one’s environment and move personal/social needs forward O Deficits can prevent people from realizing their potentials (Lal & Sanghvi, 2015)
Communication Difficulties O Slow auditory processing speed when distracted by extraneous sensory information O Interpret information literally O Difficulty with figurative language (metaphors, idioms, similes, irony) O Difficulty recognizing situations that certain vocabulary words may have alternative meanings
Communication Difficulties O Difficulty understanding the grammar and thus primarily attend to key words rather than to the message conveyed O Difficulty connecting ideas from one sentence to the next O Struggle with turn-taking
Emotional Regulation O Difficulty differentiating between O O thoughts and feelings Difficulty recognizing and labeling emotions Difficulty identifying the need to intervene on and regulate intense emotions Difficulty asking for help or responding to others’ attempts to provide support Difficulty in regulating emotions can result in heightened emotional states and undermine the development and mastery of new skills and application of previously learned skills (Volkmar et al. , 2005)
Rationale for the Program O The sexual offender population can be described as a highly diverse group that differs in terms of: O Age O Intelligence O Socioeconomic status O Antisociality O Psychiatric comorbidity
Rationale for the Program O Male sexual offenders are hypothesized to differ in relation to social competence, attitudes and beliefs about sexual offending, emotional regulation, disinhibition, poor parent -child attachment, sexual development, and history of childhood sexual abuse. O Given the heterogeneity of the sexual offender population, treatment has moved away from a “one size fits all” mentality to meeting the needs of a diverse population, including those that are diagnosed with autism.
Rationale for the Program O Sexual offender treatment requires that the participant have the ability for introspection, openly share and interact with others, which may be challenging for those with ASD.
Rationale for the Program Responsivity Principle It is the goal of the ASD-specific programming to provide a treatment modality that promotes learning, skills acquisition, and addresses core features of the disorder (e. g. , social deficits, communication problems, and problems with emotional regulation). O Will show varying levels of reactivity to the environment, self-regulation in excitable situations O Critical to use these insights when devising optimal learning environment and teaching strategies (Volkmar et al. , 2005) O
What Wasn’t Working: Residents with ASD in Regular Programming O Individuals on the spectrum seen as abrasive, uncensored, unmotivated, anxious & angry O Lack of awareness to the emotional climate in the room O Struggle to adjust facial expressions to context result in being perceived as cold O Likely to assume others hold same knowledge on various topics as them O Difficulty using nonverbals to regulate social interactions & misunderstand nuances and informal rules used in communication O Negatives experiences result in ASD individual becoming overstimulated or confused (Bumin et al. , 2015)
What Wasn’t Working: Residents with ASD in Regular Programming O Struggle to understand emotional concepts, particularly those that rely heavily on social norms (guilt, embarrassment, pride) (Volkmar et al. , 2005) O Tend to retreat into imagination or special interests O One-sided speech patterns often framed as tactile maneuvers and/or narcissism O Social problems lead to indifference, teasing, or bullying (Bumin et al. , 2015)
Portrayal of Social Rejection “We’re going to make it back to core group” Group disagreed “I don’t want to give you feedback anymore…I’m forced to give you feedback! No one has accepted my feedback. They’ve discounted me since I came to this punk ass group!” Group disagreed, we are individuals! “There’s some serious denial around here” Group disagreed Attempted to join peers, noting “we mirror one another”
Assessment for Entrance into ASD-Specific Programming: Social Responsiveness Scale (SRS-2) O School-age (ages 4 -18 years), preschool (ages 2. 5 -4. 5 years), adult (ages 19 years and older), and adult self-report O Therapists were asked to rate symptoms that they've noticed over time using a quantitative scale representing a range of severity O Five treatment subscale scores: Social Awareness, Social Cognition, Social Communication, Social Motivation, and Restricted Interests and Repetitive Behavior O Two subscales are considered DSM-5™-compatible: Scores on these subscales make it easy to compare the resident’s symptoms to DSM-5 diagnostic criteria for ASD O Settings in which residents are observed vary greatly: familiarity, degree of structure, intrusion of observer, complexity of physical environment, mode of engagement, processing demands O If factors are not considered by assessors, may result in highly discrepant views and conflicted clinical impressions (Volkmar et al. , 2005)
IDHS/TDF Participants Based on Program Type O As of January 2017, Combined Specialized Typical a total of 259 individuals are enrolled in and attend core sex offender treatment O 192 (74%) Typical O 47 (18%) Specialized O 20 (8%) ASDspecific
Development ASD-Specific Programming O Outcomes should focus on personal independence and social responsibility (National Research Council, 2001) O Curriculum and structure help by making elements of learning clearer and more predictable O Mixing new & challenging activities with familiar & motivating tasks O Emphasis on inclusion O Little research on curricula for high functioning autism O Little research for those who require education and community services through adulthood (Volkmar, et al. , 2005) O Currently, limited knowledge on adult outcomes as few studies followed individuals on the spectrum into adulthood and disorder only identified in middle of the last century (Baron-Cohen & Bolton, 1993)
Structure to ASD-Specific Programing O In addition to sex offender treatment, participants of ASDspecific programming receive weekly educational sessions that serve to increase their understanding of autism and how they differ from neurotypical individuals in the domains of: O O (a) thinking differences (b) social differences (c) emotional differences (d) sensory and movement differences (Gaus, 2011). O Participants are also taught skills to assist them in better managing their unique differences.
Structure of ASD-Specific Programing: CBT Core Concepts O Participants are expected to develop an understanding of their personal strengths and weaknesses associated with ASD and how it influences the manner in which they learn and think. O CBT concepts are introduced and taught to participants and include: O O O ABC framework Cognitive errors in thinking Irrational beliefs Rational and scientific thinking Maintenance of change O Applied Behavioral Therapy concepts O Behavioral observation, reinforcement, prompting, task analysis, chaining, fading
Structure: Learning Supports O Visual and organization supports designed to foster individual’s capacities for social communication and emotional regulation O Emphasis on the processing of written word O Decreases extraneous stimuli that may distract or confuse O Possible link between ASDs tendency to take things literally and use visualization to organize information (Volkmar et al. , 2005)
Structure: Skill Building O Development of Self- Regulation Skills O Emotional regulation can be described as the key developmental capacity associated with a persons ability to manage emotional arousal (Rothman, 2012). Difficulty with emotional regulation interferes with an individuals ability to adapt and respond to their environment in an appropriate manner. O Mindfulness Curriculum O Participants are instructed on mindfulness practices in order to increase their understanding of how differences associated with ASD contribute to difficulties in adapting to everyday life situations. O Skills development centers on teaching relaxation techniques that can be utilized to manage anxiety, working through and identifying emotions, and managing sensory issues.
Structure: Skill Building O Development of Mood Management Skills O Due to having an atypical development in emotional regulation, individuals on the autism spectrum experience difficulty in managing their emotions across different situations, remaining engaged in their social environment, and impulse control. As adults, they experience secondary difficulties with mood, anxiety, and social withdrawal (Rothman, 2012).
Skill Building: Sensory Diet O Important to teach a way to recognize when they are stressed along with a procedure for calming down (Volkmar, et al. , 2005) O Sensory balls allow individuals to emotionally regulate more independently with doses specific to their needs O Dosing provides a relaxing, focused, socially appropriate intervention O Diet provides greater control over sensory
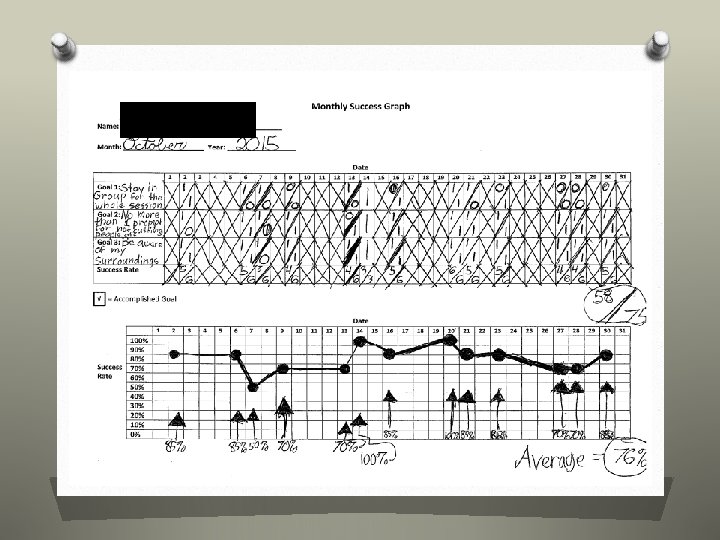
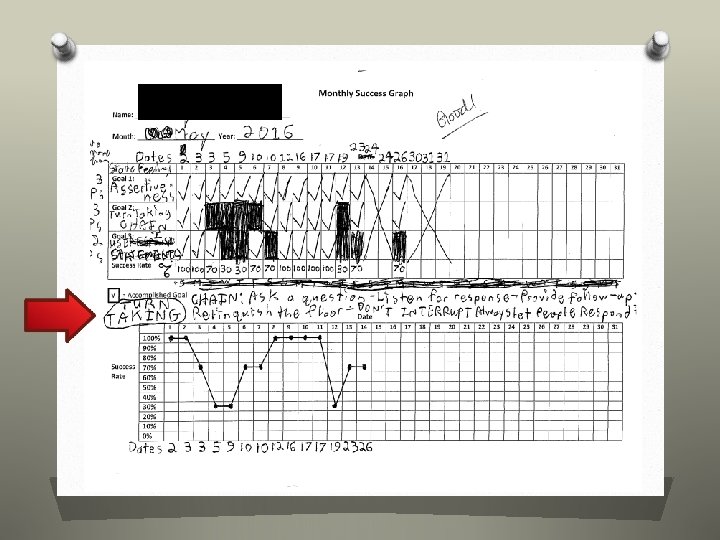
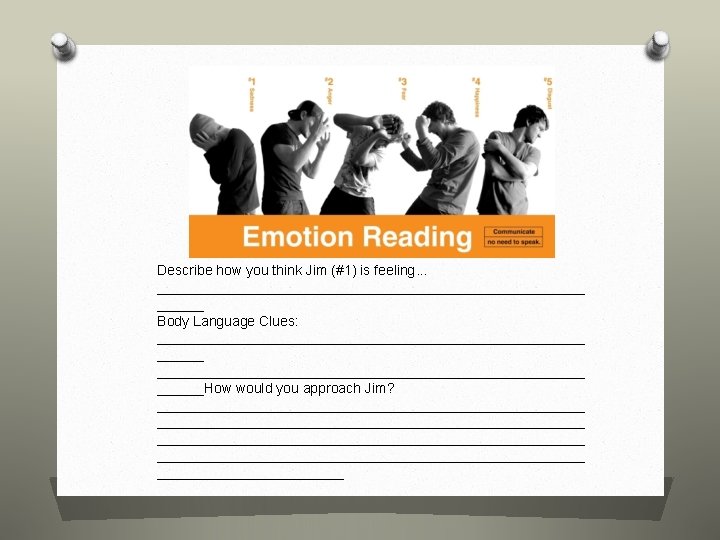
Structure: Didactic Sessions Criteria A: Social Communication/Interaction O Information Processing/thinking O O O O O differences Monthly Success Graphs What makes a successful social encounter? Emotional differences 6 Universal Emotions Range/intensity of emotions Facial Expressions Body Language Giving and receiving the nonverbal prompts of peers in group Entering/exiting conversations Physical boundaries Criteria B: Restricted Behavior O Sensory/Movement O O difference Sensory Diet Monthly Success Graphs Problem-Solving Mindfulness course
Structure to Combined Programing: Future Development Social Skills Curriculum O Addresses social deficits that are associated with ASD. The participants are taught skills and are provided with the opportunity to rehearse skills in the following areas: O Conversational Skills O Building Relationships O Managing Social Rejection O Working Through Conflict Vocational Curriculum O Assists participants in developing vocational skills with an emphasis on addressing common problems encountered by the ASD population. O Social Understanding of Work Environment (e. g. , rules, behavioral expectations, and boundaries) O Decision Making Skills O Managing and Reducing Anxiety
Case Example #1 Mr. S. ’s difficulties with emotional regulation and sensory issues were interpreted by facilitators and his peers as disrupting to the group process: “Annoying” “bothersome” “struggles with assertiveness” Benefits of Combined Programing Mr. S. has shown improvement with his ability to regulate his emotions. When Mr. S. was asked regarding his experience in the Combined Group, he stated, “You can help each other with the different type of challenges in that phase. ” Mr. S. also reported that it was “fun” due to the different activities and were offered.
Resident’s goal: “Not to cut people off” Actual social significance of the behavioral target is to improve his adherence to invisible rules of conversation
The case of Mr. J Before ASD-Specific Programming …not utilized available alliances effectively, and has typically shown no initiation in seeking out support or direction. . Mr. J consistently demonstrates a significant lack of participation in group process…. He does not independently participate in group discussions, or offer any feedback to others. What feedback he does provide when prompted tends to be brief, and vague or superficial in nature… …Tactics such as diversion, silence, or casing in response to feedback or challenges from others… He often agrees with feedback from others, without apparent consideration of the actual point being made, in an effort to avoid discussion or challenges… …begins focuses by making inflammatory statements designed to elicit copious feedback from the group, after which he allows the group to use his focus time responding to his statements, and thus avoids actually processing his own issues. After ASD-Specific Programming Mr. J appears comfortable discussing intimate life details as well as treatment and facility challenges. Mr. J has struggled with the quality of his participation in Combined Group. He has attributed his lack of participation to difficulty relating to the topics other group members discuss.
The case of Mr. B Before ASD-specific Programming. After ASD-specific Programming …appeared uninvested in the group process, as evidenced by avoiding eye contact, closed posture and showing little reaction to what is being talked about. Mr. B arrives early to group and typically presents with good eye contact and open body language. Though he is a quieter group member, he is often observed nodding or shaking his head, thus he appears to consistently be following group discussions. He will offer tactful feedback when pulled into conversations by peers or therapists.
The Case of Mr. D. Before “Constant humiliation” After “No matter what I’m saying people can relate. ”
ASD Programming & Decreases in Rule Violations 5 # of Rule Violations 4 3 Major 2 Minor Warning 1 0 6 201 5 201 3 201 1 201 0 201 Year 9 200 8 200 7 200 6 200
Maladaptive Posture of Treatment Provider scrutinizes client for disruptive behavior Client dysregulates Client becomes more anxious Provider responds sharply Instructs client to stop
Tips for Providers
Summary of ASD Client’s Difficulties: Theory of Mind O The ability of a person to recognize and comprehend the thoughts, beliefs, desires, and intentions of other people O Difficulty recognizing and processing the feelings of others O Difficulty understanding the different perspectives of others O Difficulty interpreting if behaviors are intentional (Edelson, S. M. , 2017)
Posture of the Treatment Provider when Engaging with Clients on the Spectrum O Patience & sensitivity to person’s unique symptoms O Cautious in terms of nonliteral speech (metaphors, irony, sarcasm, humor) O Generalizing treatment gains remains an obstacle (Volkmar et al. , 2005) O Strength finder O Assist in skill development rather than correction of social mistakes (Laugeson & Frankel, 2010) O Utilizing special interests to engage https: //vimeo. com/171179837
Posture of Treatment Provider O Use of modeling to teach Provider responds in a manner to lessen the anxiety Provider considers what he must be feeling Client dysregulates social skills to teach spontaneous social interaction in natural settings (Volkmar et al. , 2005) O Social coaches are competent in addressing repeated misbehavior, discussing conflict resolution, modeling desired skills, performance feedback (Laugeson & Frankel, 2010)
Future Direction O Screening methods O Distinguishing psychopathy & NPD from ASD O Ways to target vocational success O Reintegration into the community
Special Thanks Dr. Darren Matusen, Psy. D.
References American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5 th ed. ). Washington, DC: American Psychiatric Association. Baron-Cohen, S. & Bolton, P. (1993). Autism The Facts (pp. 79). New York. Oxford University Press. Bumin, G. , Huri, M. , Salar , S. , & Kayihan, H. (2015). Occupational Therapy in Autism, Autism Spectrum Disorder Recent Advances, Prof. Michael Fitzgerald (Ed. ), In. Tech, DOI: 10. 5772/59168. Available from: http: //www. intechopen. com/books/autism-spectrum-disorder-recent-advances/ occupational-therapyinautism (pp. 174). Edelson, S. M. (2017). Theory of Mind. Autism Research Institute. Available from https: //www. autism. com/understanding_theoryofmind. Gaus, V. (2011). A Unique Brain. In, Living Well on the Spectrum (pp. 9 -57). New York, NY: The Guilford Press. Lal, R. & Sanghvi, D. (2015). Autism and Functional Language Development – An Experiment with AAC Intervention, Autism Spectrum Disorder - Recent Advances, Prof. Michael Fitzgerald (Ed. ), In. Tech, DOI: 10. 5772/59137. Available from: http: //www. intechopen. com/ books/autism-spectrum-disorder-recent-advances/autism and-functional-language-development-an-experiment-with-aac-intervention (pp. 205). Laugeson, E. & Frankel, F. (2010). Social Skills for Teenagers with Developmental and Autism Spectrum Disorders: (pp. 45). The PEERS Treatment Manual. Routledge. National Research Council. (2001). Education children with autism (Committee on Educational Interventions for Children with Autism, Division of Behavioral and social Sciences and Educations) (p. 40). Washington, D. C: National Academy Press. Rothman, D. (2012). Autism Spectrum Disorders and Sexual Behavior Problems. In, The Sex Offender, Current Trends in Policy and Treatment Practice (pp. 26 -1 - 26 -23). Kingston, NJ: Civic Research Institute. Shriber L. 2010. Autism: A Neurological and Sensory Based Perspective. In: JH Stone, M Blouin, editors. International Encyclopedia of Rehabilitation. Available online: http: //cirrie. buffalo. edu/encyclopedia/en/article/285/ Torun, Y. , Gu ney, E. , & Iseri, E. (2015). Structural and Functional Brain Imaging in Autism Spectrum Disorders, Autism Spectrum Disorder - Recent Advances, Prof. Michael Fitzgerald (Ed. ), In. Tech, DOI: 10. 5772/59121. Available from: http: //www. intechopen. com/books/autism-spectrum-disorderrecentadvances/structuraland-functional-brain-imaging-in-autism-spectrum-disorders (pp. 41). Volkmar, Fred et al. , eds. (2005). (pp. 774 -775, 778, 782, 870, 875, 887, 940, 982, 996, 1017). Handbook of Autism and Pervasive Developmental Disorders. 3 rd ed. Hoboken, NJ: John Wiley & Sons, Inc. Wilkinson, L. (2015). Adults on the Autism Spectrum. In, Overcoming Anxiety and Depression on the Autism Spectrum (pp. 914). London, UK: Jessica Kingsley Publishers.
Appendices
Monthly Success Graph Name: ____________________ Month: __________ Year: _________ Date 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 Goal 1: Goal 2: Goal 3: Success Rate √ = Accomplished Goal Succes s Rate 100% 90% 80% 70% 60% 50% 40% 30% 20% 10% 0% 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31