A LIFELONG REMEMBRANCE OF THAILAND PARAPARESIS AS SEQUELAE

A LIFELONG REMEMBRANCE OF THAILAND – PARAPARESIS AS SEQUELAE OF NEUROLOGICAL MELIOIDOSIS Andrea Lenger 1 Friederike Asboth 2 Oskar Janata 1 1 Infection Control Team, 2 Institute for Pathology – SMZO Danube Hospital Vienna, Austria

History q Viennese man, 54 a, presents with increasing weakness in both legs since two days q Sudden stabbing pain in the left thigh 3 days ago while walking q Weakness in both lower extremities on the next morning, now unable to walk q No preexisting relevant medical conditions, no medications, no recent vaccinations q Longtime alcohol consumption of ca. 1, 5 l wine/d, 60 cigarettes/d q No recent febrile illnesses q No travelling abroad in the last 6 months - but several weeks in Thailand 8 months ago in the rainy season !

Neurological Status q Patient awake, orientated, no meningism q Cranial nerves normal; Upper extremities: normal on both sides q Lower Extremities - Muscle Strength Grades ü Hip : Flexion 1 bil. , Extension 0 -1 bil. , Adduction, Abduction 0 -1 bil. ü Knee : Flexion right side 3 -4, left 0 -1, Extension 0 -1 bil. ü Foot : Elevation right 3 -4, left flaccid paresis, Plantarflexion right 4, left flaccid paresis q Tendon reflexes : Patellar left >right, Achilles weak bil. , Babinski, Lasegue neg. bil. ; no cloni, no spasticity q Sensitivity : hypoesthesia from distal third of lower leg, no sensitivity for vibration
 Ä")
Diagnostic Work Up q Laboratory Results Ä CRP 19, 6 mg/l ( 5) Ä CK 3470 U/L, CK-MB 54 U/L Ä LDH 369 U/L Ä ALAT 59 U/L, GGT 90 U/L Ä Na 125 mmol/L, K 3, 1 mmol/L q CSF- Puncture Ä White blood cell count 318/microl, Glucose 28 mg/dl, Lactat 5. 8 mmol/L, Totalprot. 1636 mg/L, Albumin 916 mg/L Ä 80 -90 % neutrophile granulocytes, activated lympho- and monocytes, multiple leucophages, some phagocytes with signet ring cell morphology Ä Gram stain : no bacteria q MRI of the Spine
 T 2")
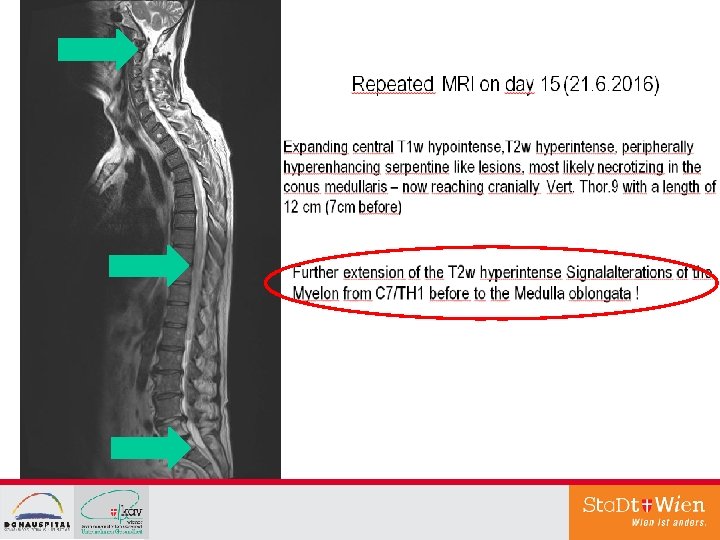
MRI of the Spine on the day of Admission (6. 6. 2015) T 2 weighted hyperintense signalalteration of the myelon from the middle thoracic region caudally to the conus, partly of the whole diameter, in the caudal parts more dorsally situated. After Application of contrast mainly enhancement in the cranial parts and in the proximal roots close to the conus. Summary : Picture of a transverse myelitis of the lower thoracic myelon and the conus; the enhancement rather excludes an acute vasculitis. No typical signs of Encephalitis Disseminata, also no typical markers for ADEM - especially no cerebral involvement.
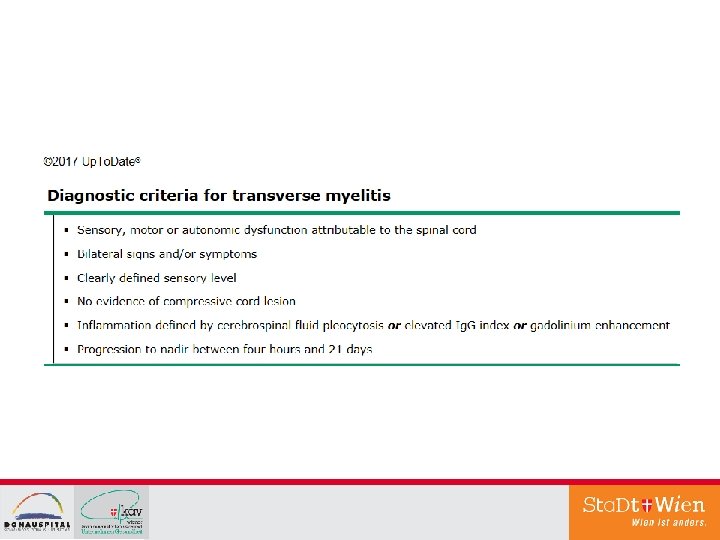

Differential Diagnoses of the Neurologists Ø Transverse Myelitis Ø Ø bacterial or viral pathogens Tuberculosis of the CNS Parainfectious Parasites Ø Autoimmunologic disease – Vasculitis ? Ø Paraneoplastic? Ø (MS; Neuromyelitis optica)

Initial Therapies - polypragmatic q Ceftriaxon & Acyclovir q From the 1. day antituberculous drugs (Rifampicin, INH, Ethambutol, Pyrazinamid) q 5 days Methylprednisolon 1 x 1 g/d q Plasmaphereses (day 9 -12)
 positive")
Many Results from the Lab… q Many bloodcultures – negative q Quantiferon (IGRA) positive q CSF- Cultures – negative q CSF-PCR Biofire Meningitis – negative q Broadspectrum – PCR from CSF (bacterial and fungal) negative q TBC-PCR, ZN negative (3 x in CSF and urine) q Marker for antibody mediated autoimmunological diseases of the CNS in CSF/Serum negative q CA 19 -9 118. 6 k. U/l (-37) CEA 12. 8 k. U/l (-5) q TBC-Cultures pending …. q Virus – PCR (HSV, VZV, Enterovirus, CMV, Adeno, HHV 6, PVB 19) neg. q Mycoplasma pn. PCR neg. q Borrelia - Serology (ELISA) neg. q Serology for Parasites (Cysticercosis, Toxocara, Ascaris, Trichinella) negative

„Optimization“ of the initial Therapies polypragmatic
 because of respiratory insufficency")
Intervention q Transfer to the ICU on day 30 (!) because of respiratory insufficency q Neurosurgical intervention on the same day: Ä Opening of the Dura Mater at TH 10/11 : no abscess Ä TH 9/10 : Pus intramedullary – suction, flushing q Finally material for the labs !

Therapy & Outcome q 6 Weeks Ä Meropenem 3 x 2 g iv + Trimethoprim/Sulfamethoxazol 3 x 160/800 mg iv q 6 Months Ä Trimethoprim/Sulfamethoxazol 160/800 mg 2 x 1 p. o q 7 Weeks ICU, then 8 weeks at the neurologic ward, thereafter transfer to neurorehabilitation Ä Sustained Paraplegia with good function of the arms Ä Mobility in wheelchair autonomously Ä Urinary and faecal incontinence

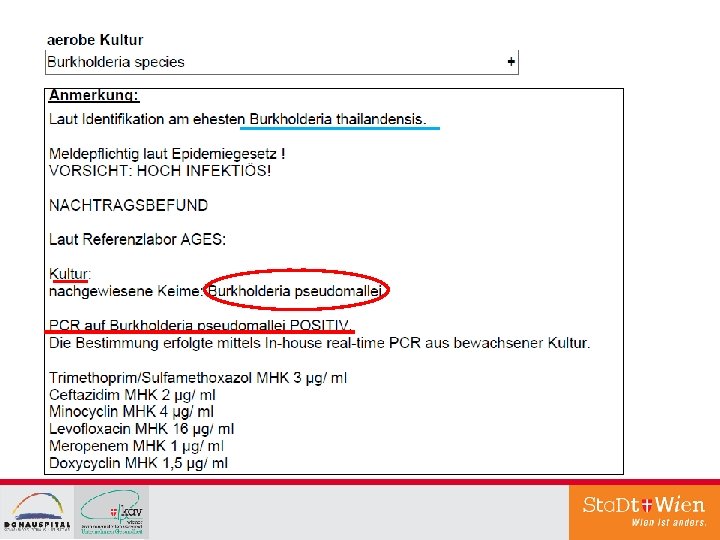
Neuromelioidosis q Pathogen: Burkholderia pseudomallei – aerobe gramnegative bacillus q Occurrence: in soil and water mainly in Southeast Asia and the Northern Territories of Australia q Transmission: percutane inocculation, inhalation, ingestion, ev. aspiration – mainly during the rainy season q Many infections asymptomatic, 85% acute disease after recent infection (incubation period mostly ca. 1 -21 d), 11% chronic, very rarely reactivation of a latent infection – longest reported latency 62 years ! q Organmanifestations: mainly lungs, urogenitary system, skin / soft tissues – very rarely CNS - then with high mortality; bacteremia, frequently abscesses in various organs, septic shock in ca. 25% q Riskfactors: alcoholism, diabetes, chronic lung- and renal diseases
- Slides: 15