A lady with status epilepticus Dr Alfred YF

 § § § 47 year-old housewife NDNS, deny substance abuse Epilepsy but")
 § Attend AED on 24/2/2005 midnight § Complain generalized bone pain and")












")
N, N-dimethyl-a -(2 -methylpropyl)-, hydrochloride, monohydrate")




 but vital sideeffects § § § General: anaphylaxis; Musculoskeletal: myalgia, hypertonia Cardiovascular:")




 § No specific recommendation § Prevent absorption by gastric")










- Slides: 43
A lady with status epilepticus Dr Alfred YF Chan ICU Friday Seminar 11/8/2006
History (1) § § § 47 year-old housewife NDNS, deny substance abuse Epilepsy but defaulted FU for decades, not on any anti-epileptics § Feb 2005, talk in irrelevant content for ~ one week, getting increasing agitated
History (2) § Attend AED on 24/2/2005 midnight § Complain generalized bone pain and limb weakness for 3/7 § Claimed to have “leukemia” after “bone marrow examination” done by PY doctors § No fever, no flu contact, no travel history § AED decision admit medical for investigating bone pain
Examination § § § GCS E 4 V 5 M 6, orientated but “anxious” Pulse 100/min, BP 158/88 PERL, trace of gum bleeding seen Increased limb muscle tone. 4 limbs power 4/5 limited by pain. Reflex/ sensation normal § CVS/ Chest/Abdomen NAD
Impression § § § Working diagnosis: polymyositis? CT brain: no abnormality seen CK 68; WCC 10. 4 (Neutrophil 7. 9); TSH 2. 89; LFT and electrolytes all normal § ECG showed SR 100/min, QRS 76 ms, QTc 345 ms. No ischemic change § Treatment: BDZ, Dologesic PRN for pain
Progress----Day 2 § Delusion of getting “leukemia” persisted § Seen by psychiatry for ? psychosis took propriety drug from China since Chinese New Year (Last pill ~1 week) impression of drug-induced psychosis? § Serum/ urine for toxicology § Trace private drug for identification
Progress----Day 3 § Urine toxicology: identified Propoxyphene, N-desmethyl propoxyphene § Panadol/ salicylate/ alcohol levels normal § Increased violence, on Haldol 1. 5 mg N § Muttering to air e. g. “I am a man” § Private drug A/V: weight reduction pill § Decision: re-consult psychiatry
Progress----Day 4 § § § § Right upper limb twitching 0045 Generalized tonic-clonic convulsion 0540 Comatose at 0640 Intubated at ward for second CT brain normal again Bolus Dilantin IV 750 mg at 0650 Convulsion again at 0800 To ICU for further care
Serial blood results 25/2 28/2 1/3 2/3 CK 68 1440 52600 61800 Creatinine 69 200 329 408 p. H N/A 7. 39 7. 22 7. 19 BE N/A -11. 5 -16. 4 -18. 0 Platelet 262 196 39 32 INR/APTT N/A <1/37 <1/34 <1/36
Progress----further workup at ICU § § § Peripheral smear: no fragmented RBC Bedside USG abdomen: NAD Weil-Felix serology; Leptospira Ig. M; Hanta virus antibody all subsequently normal ANF/ RF/ C 3 & C 4/ ANCA all negative Blood culture/ urine/ sputum no growth EEG predominant slow waves seen
Lumbar puncture § § § § Opening pressure 10 cm H 2 O Protein 0. 42; glucose 4. 7 (serum 6. 0) Cell count: RBC 0; WCC 0 Gram stain/ AFB smear/ Indian ink negative CSF VDRL negative CSF showed no malignant cells CSF for JBV, other viral studies T/F
Progress---- supportive care at ICU § Airway, ventilation, inotropes § Forced alkaline diuresis: (300 ml 8. 4% Na. HCO 3 in 2 L H 2 O) at 200 ml/ hour + Lasix infusion at 10 mg/ hour. § Aim at urine output >100 ml/ hour § Thiopentone coma: 1 to 5 mg/kg/hour § Anticonvulsant: dilantin/ tegretol § Empirical IV Acyclovir
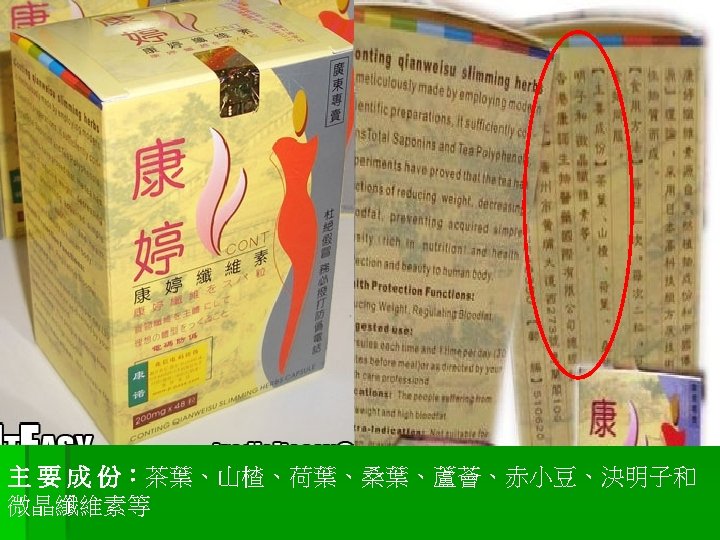
Support, but what had happened? CNS dysfunction with thrombocytopenia § Thrombotic thrombocytopenic purpura § SLE +/- anti-phospholipid syndrome § Haem malignancy with CNS involvement § Viral encephalitis e. g. Japanese B § Aseptic meningoencephalitis e. g. Ricketsia § 康婷纖維素( Drug sent to TRL on ICU D 2)
Drug induced seizure § Amphetamines, Anticholinergics, Aminophylline § Bupropion § Camphor, Carbamazepine, Cocaine, Cyanide, Carbon monoxide § Hypoglycemics Status epileticus § Isoniazid, Insulin § Lidocaine § Organophosphates § Phenytoin § TCA, Tetramine § Withdrawal (Alcohol, BDZ)
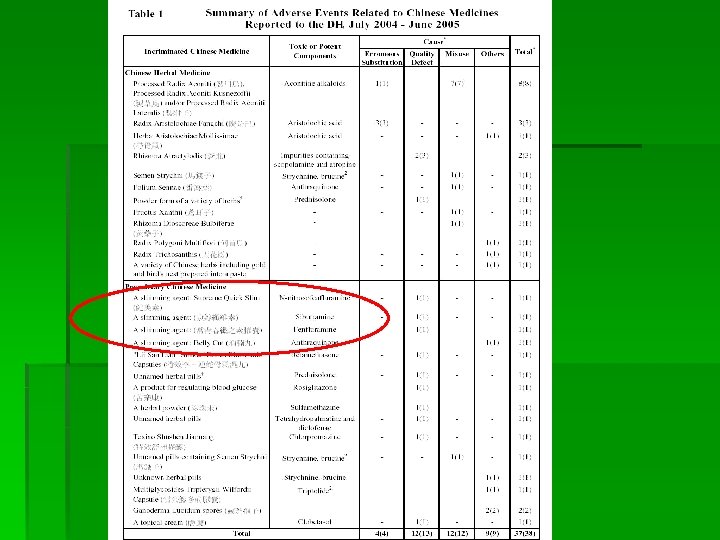
ICU Day 10 § Analysis from TRL Sibutramine isolated from 康婷纖維素 § Confirmed (1) drug induced seizure, & (2) Chinese medicine containing Western drug Notify Chief Pharmacists Office (CPO) & Central Notification Office (CENO) of Department of Health (DH)
Sibutramine Cyclobutanemethanamine, 1 -(4 -chlorophenyl)N, N-dimethyl-a -(2 -methylpropyl)-, hydrochloride, monohydrate
Sibutramine action § Inhibit reuptakes of Noradrenaline, serotonin, Dopamine at synapses § Thermogenic effects § No pre-synaptic neurotransmitter release (Compare to Fenfluramine) § Metabolized at liver led to 2 active metabolites , M 1 and M 2
Sibutramine pharmacokinetics § § § Rapid absorption after ingestion Extensive first-pass effect at liver 97% bound to serum protein Metabolized by P 450 at liver 85% excreted in urine
Clinical use of sibutramine § § § FDA approval: November 1997 Appetite suppressant via hypothalamus Significant weight loss with sustained benefit up to 2 years Better lipid profiles (lower TG, raise HDL) ? improved glucose tolerance Dose: 10 mg QD, maximum 15 mg QD
Common side-effects: mild ~1% ~18. 6%
Rare (<1%) but vital sideeffects § § § General: anaphylaxis; Musculoskeletal: myalgia, hypertonia Cardiovascular: VT; Serotonin syndrome Gastrointestinal: cholelithiasis, GI bleed Haematological: Thrombocytopenia CNS: abnormal thinking; nightmare; seizure
Important drug interactions § Mono-amine oxidase inhibitors MAOI § Selective serotonin reuptake inhibitor SSRI § NA reuptake inhibitor e. g. Effexor § TCA e. g. amitriptyline, imipramine § Dopaminergic e. g. L-Dopa; Bromocriptine § “Street drug” e. g. LSD, MDMA § Drugs inhibit cytochrome P 450
Our lady got the following reported side-effects § § § High blood pressure, tachycardia Myalgia, limb hypertonia Anxious, insomnia, hallucination Gum bleeding (platelet dysfunction) Thrombocytopenia Seizure
Seizure related to Sibutramine § In the largest clinical efficacy trial, 2068 individuals on Sibutramine compared to 884 people on placebo § Only 3 subjects on Sibutramine developed seizure (0. 1%). Two of them had known history of epilepsy § ? Only affect vulnerable subjects
My hypothesis § Sibutramine induced serotonin syndrome as a result of co-administration of other drugs, which were not identified in history § Status epilepticus in susceptible individual with high serotonin tone
Manage Sibutramine overdose (POSINDEX 2006) § No specific recommendation § Prevent absorption by gastric lavage and activated charcoal as appropriate § Consider Labetalol for significant cardiovascular manifestation or clinical status mimicking Serotonin Syndrome § Seizure control
Overdose Sibutramine---scanty reports § Acute overdose of 100 mg in a 30 -year-old male resulted in no adverse effects or ECG abnormalities (Prod Info Meridia(R), 1999) § Acute overdose of 400 mg in a 45 -year-old male caused sinus tachycardia at 120/ min. No other adverse effects were reported (Prod Info Meridia(R), 1999) § In a toxic surveillance study, 8 adults ingested a median amount of 30 mg Sibutramine. Tachycardia, hypertension and dizziness were seen. Symptoms were not life-threatening and no mortality occurred (Mrvos et al, 2000).
Fluid strategy § Ideal fluid is half isotonic saline with Na. HCO 3 added, e. g. 1 L normal saline + 1 L D 5 + 100 mmol Na. HCO 3. § Give at least 3 -6 L/ day, may be up to 10 L § Add mannitol infusion at 10 ml/ hour if urine >20 ml. / hour
Progress after ICU admission § Day 3: repeat EEG NAD; thiopentone off § Day 5: complicated by VAP by Klebsiella, IV Claforan was given for 7 days § Day 9: extubated § Day 10: skin rash developed. Drugs switched to Luminal/ Keppra/ § Day 14: D/C general ward § Day 21: RFT back to baseline
Highlights in this case § § § Psychiatry for history taking? Organic cause for acute onset delusion? Recognition of Serotonin syndrome Seizure management Toxidrome (toxication syndrome) analysis: seizure, bradycardia, tachycardia, hypothermia § Investigation for sake of public alert
What is the situation in Hong Kong about Sibutraminerelated incidents?
Center of health protection § Had issued warnings about presence of Sibutramine in multiple “health products” and “slimming pills” § 4/8/2005: 美盈素; § 26/8/2005: 消腩丸 § 7/9/2005: 康婷纖維素 § 2/12/2005: 美姿纖維素
Sibutramine Still in big stock and sale
What do products contain to promote sliming? § § § Laxatives: TCM; Phenophalein Diuretics: thiazides Appetite suppressant: Fenfluamine/ other amphetemine derivatives; Sibutramine Hormonal: thyroxine; animal thyroid gland extracts Anti-absorptive: Xenical Other: caffeine; beta-blocker; anxiolytics
Easier and safer method to lose weight