A Guide to Red Blood Cell Indices Mary

A Guide to Red Blood Cell Indices Mary Ann Thompson, M. D. , Ph. D. May 8, 2013
 WBC # n RBC # n Hemoglobin n Hematocrit n")
Complete blood count (CBC) WBC # n RBC # n Hemoglobin n Hematocrit n RBC indices: MCV, MCHC, RDW n Platelets n
 x 10/ RBC ct")
RBC indices n MCV: mean corpuscular volume ¨ Hct (%) x 10/ RBC ct (x 106/ml) n MCH: mean corpuscular hemoglobin ¨ Hgb (g/d. L) x 10/ RBC ct (x 106/ml) n MCHC: mean corpuscular Hgb conc. ¨ Hgb (g/d. L) x 100/ Hct (%) n RDW: rbc distribution width
 RDW-SD is measured at the")
XE-Series Principles and Technology Red Cell Distribution Width (RDW) RDW-SD is measured at the 20% relative height of the curve RDW-CV can be falsely elevated or decreased depending on the MCV since MCV is in the denominator

RBC indices n MCV: mean corpuscular volume ¨ Nl 81 -98 f. L ¨ Gauge of microcytic, normocytic or macrocytic anemia n MCH: mean corpuscular hemoglobin ¨ Nl 27 -32 pg n MCHC: mean corpuscular Hgb concentration ¨ Nl 31 -35 g/d. L ¨ High in spherocytosis ¨ High if Hgb spuriously high due to interference (turbidity, TPN, etc. )

RBC indices n RDW: rbc distribution width ¨ RDW-SD nl 37. 4 -52. 4 f. L ¨ RDW-CD nl 11. 1 -14. 3% ¨ High in iron deficiency anemia
 / 45 n Reticulocyte")
Corrected Reticulocyte Count = Percent Observed Reticulocytes x Patient’s Hematocrit) / 45 n Reticulocyte Production Index= n [(Percent Reticulocyte x Hematocrit Value)/45] x [1/Correction Factor] n

Correction Factor Pts. Hematocrit Value, % Correction Factor 40 -45 1. 0 35 -39 1. 5 25 -34 2. 0 15 -24 2. 5 <15 3. 0

Causes of Microcytic/hypochromic Anemia n Deficient Hemoglobin Synthesis ¨ Iron ¨ Protoporphyrin ¨ Globin

Common Causes of Microcytic Anemia Iron deficiency • Anemia of chronic disease • Thalassemia minor •

Causes of Microcytic Anemia n Disorders of iron metabolism ¨ Iron deficiency ¨ Anemia of chronic disease n Disorders of heme synthesis: Sideroblastic anemia ¨ Hereditary ¨ Acquired idiopathic (myelodysplasia) ¨ Acquired toxic (lead, drugs, alcohol) n Disorders of globin synthesis: Thalassemias

Ddx of Microcytic/hypochromic anemia Smear review: no diagnostic changes Nl RDW, Nl or Hi RBC #: Suspect early iron deficiency, thalassemia, or Abnormal hemoglobin Nl RDW, Low RBC#: Suspect anemia of chronic disease Hi RDW (> 16): Suspect iron deficiency anemia Hb. A 2 level Serum ferritin Additional iron tests Bone marrow exam Serum ferritin Additional iron tests >4%: Beta-thalassemia <4%: Hemoglobin analysis Low ferritin: Iron deficiency High ferritin Bone marrow exam Sideroblastic anemia Marrow failure
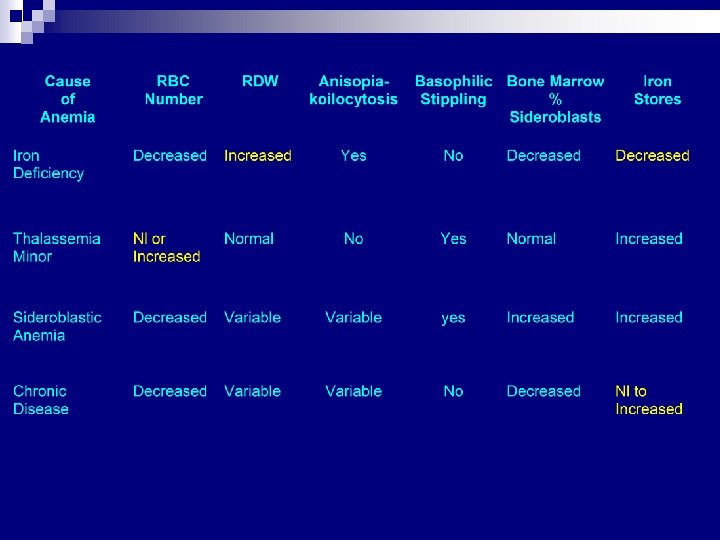

Ddx of Thalassemia minor vs. Iron deficiency anemia n n n In thalassemia, MCV and MCHC < than those in same degree of iron deficiency anemia Microcytosis with RBC > 6 x 106/ul suggests thalassemia MCV/RBC <13 in Thalassemia minor, >13 in iron deficiency anemia Basophilic stippling and target cells common in thalassemia RDW nl in thalassemia minor, high in iron deficiency anemia

b-thalassemia major

Detection of b Thalassemia trait n n n Rathod, D. et al Usefulness of cell counter-based parameters and formulas in detection of b-thalassemia trait in areas of high prevalence AJCP 128: 585, 2007 Sensitivity and specificity of parameters and formulas for detecting b -thal and b-thal + IDA Winner: Shine and Lal Index: MCVx. MCH/100 ¨ n For b-thal sensitivity 99. 01%, specificity 93. 3% with cut-off of <1, 530, for b-thal + IDA sensitivity 94. 8%, specificity 70% Runners-up MCV ¨ MCH ¨ Srivastava index: MCH/RBC ¨ Mentzler index: MCV/RBC ¨
 Serum iron and")
Ddx of Iron Deficiency Anemia vs. Anemia of Chronic Disease (ACD) Serum iron and % saturation low in both n TIBC hi in iron deficiency, low in ACD n Serum Ferritin low in iron deficiency, nl or high in ACD n Marrow stores absent in iron deficiency, high in ACD n

IRON STUDIES IN HYPOCHROMIC ANEMIAS

Case 1 18 month old male admitted for FUO n CBC: n ¨ WBC 22. 9 K/ml ¨ PCV 20% ¨ Hgb 5. 3 g/d. L ¨ Platelets 700 K/ml n Differential: 40% neutrophils, 47% lymphocytes, 7% monocytes

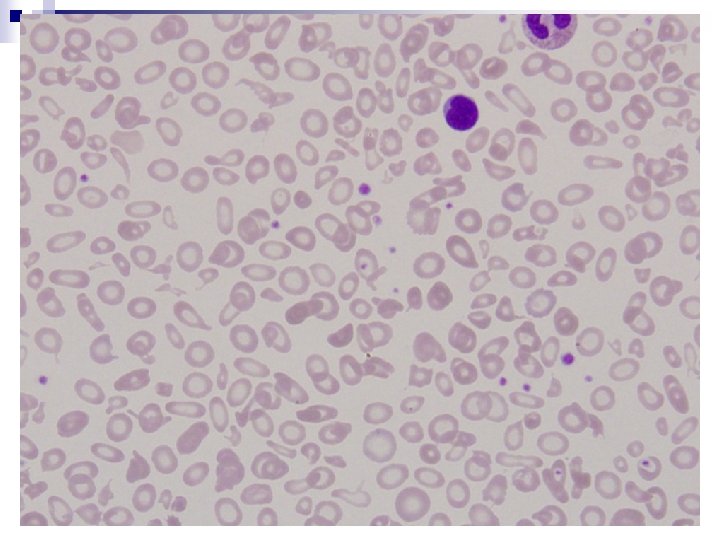
Case 1

Case 1 n RBC indices: ¨ MCV 52. 1 f. L ¨ MCH 24. 2 pg ¨ MCHC 27. 3 g/d. L ¨ RDW 21. 7% ¨ RBC 3. 76 mil/ml ¨ 2% reticulocytes
 ¨")
Case 1 n Iron studies ¨ Serum iron 6. 0 mcg/d. L(50 -150) ¨ TIBC 483 mcg/d. L(250 -450) ¨ Ferritin 6. 1 ng/m. L(10 -300) n Diagnosis: Iron deficiency anemia

Case 2: Lab values n n n n n WBC = 9. 1 K/ml Hb = 9. 6 g/d. L PCV = 30% Plts = 481 K/ml RBC = 6. 68 mil/ml MCV = 45 MCH = 14. 4 RDW = 27. 3 Reticulocyte = 1. 0%


Case 2 1 year ago RBC indices were normal n Thalassemia vs. Iron deficiency ? n Iron deficiency n ¨ History ¨ High RDW ¨ Increased plts n MCV/RBC = 8. 87—thalassemia?

Hemoglobin evaluation Hb. A 75% Hb. F 2% Hb. E 23% Hb. A 2 cannot be quantitated since Hb. E elutes similarly
 n Second most prevalent Hb variant")
Hemoglobin E Hb E is b 26 (Glu—Lys) n Second most prevalent Hb variant n >80% in Southeast Asians n 19% incidence in refuges from Cambodia and Laos n Mutation creates a cryptic donor splice site that competes with the normal donor splice site n

Hemoglobin E n Hb AE trait ¨ Clinically silent ¨ Microcytosis, MCV = 65 ¨ Slight erythrocytosis ¨ No significant anemia ¨ 20 -35% E due to poor synthesis (due to splice site competition), and m. RNA instability n Hb. E homozygous ¨ Thalassemia-like due to poor synthesis ¨ MCV 55 -65

Hemoglobin E n Relative proportion of Hb E decreases if concomitant a thalassemia ¨ Poor competition with normal b chains if a chains limiting n Reduced Hb E if iron deficiency

Case 3 n 20 month old male with severe anemia.

Case 3 Lab values WBC=21. 7 K/ul n PCV=24% n Plts =354 K/ul n MCV= 49 f. L n RBC= 4. 89 mil/ul n MCH= 17 pg, MCHC= 34. 6 g/d. L n RDW= 30. 3%, n Reticulocyte count= 1. 6% n
")
Case 3 supplemental data n Iron studies ¨ Iron 93 mg/d. L(50 -120 nl) TIBC 211 mg/d. L (250 -450 nl) ¨ % sat 44 ¨ Ferritin 402 ng/m. L (10 -300 nl) ¨

Case 3 n HPLC results ¨ Hemoglobin A 90. 8% ¨ Hemoglobin A 2 1. 8% ¨ Hemoglobin F 1. 2% ¨ Hemoglobin other 6. 2%

Case 3 Isoelectric focusing

Isoelectric focusing gel electrophoresis

Case 3 Diagnosis n Alpha-thalassemia

Normal Hemoglobins in Adults Hb. A: a 2 b 2: ~98% n Hb. A 2: a 2 d 2: 1. 5 -3. 5% n Hb F: a 2 g 2: <1. 0% n

Hereditary Spherocytosis: Labs Chronic extravascular hemolysis n Increased MCHC (>34 g/d. L; due to decreased surface area) n Increased osmotic fragility n Coomb’s test to rule out autoimmune hemolytic anemia as cause of spherocytosis n
 ¨ Promyelocytes,")
New parameters of the Sysmex XE-5000 n IG: Immature granulocytes (%, #) ¨ Promyelocytes, metamyelocytes IPF: Immature platelet fraction (%) n IRF: Immature reticulocyte fraction (%) n Ret-He: Hemoglobin content of reticulocytes n

Immature platelet fraction IPF measures platelets newly released from bone marrow n Therefore IPF is a measure of the rate of thrombopoiesis n www. healthsystem. virginia. edu/internet/hematology

Immature platelet fraction n n Ratio of immature platelets to total number of platelets The reticulocyte channel utilizes a fluorescent polymethine dye that recognizes RNA and DNA ¨ Separates reticulocytes from rbcs based on cytoplasmic RNA ¨ Separates immature platelets based on amount of RNA ¨ The highly fluorescent immature platelets are defined as those with the highest 3% intensity of fluorescence ¨ Nl 0. 9 -7%
 Reticulocyte channel histograms Fluorescence intensity (RNA/DNA) Mature platelets Immature platelets")
Forward scatter (cell volume) Reticulocyte channel histograms Fluorescence intensity (RNA/DNA) Mature platelets Immature platelets

Immature platelet fraction Briggs, C. et al Br J. Haematol. 126: 93, 2004

Uses of the IPF n Evaluation of thrombocytopenic patients ¨ Distinguish between increased platelet destruction and decreased platelet production n Prediction of the recovery phase of thrombocytopenia ¨ Regeneration after chemotherapy ¨ Engraftment after bone marrow transplant

Role of the IPF in diagnosis of ITP Confirm that thrombocytopenia is due to increased destruction rather than ineffective thrombopoiesis n Including IPF in work-up is cost-effective, as it is automatically run in the reticulocyte channel n In atypical cases or cases that are refractory to treatment, will this avoid bone marrow biopsy for the patient? n

IPF and platelet transfusion assessment

Briggs, C. et al. , Br J. Haematol. 126: 93, 2004

Rise in IPF precedes engraftment Takami, A. et al. Bone Marrow Transplantation 39: 501, 2007

Immature Reticulocyte Fraction “The reticulum” is a mixture of RNA and protein n Fluorescent dye directed against RNA binds to the reticulum. n Reaction uses same reagents as the usual reticulocyte channel n

Immature Reticulocyte Fraction n Reticulocytes divided into 3 fractions based upon the amount of fluorescence detected in the reticulocyte cytoplasm ¨ LFR: Low fluorescence reticulocyte ¨ MFR: Medium fluoresence reticulocyte ¨ HFR: High fluoresence reticulocyte IRF= MFR + HFR n Nl 2. 6 -20. 4% n

Immature Reticulcyte Fraction

www. beckmancoulter. com/literature/Clin. Diag/recticliterature. pdf

Ret-He or CHr Measure of hemoglobin in the reticulocyte n Nl 29. 8 -40. 4 pg n Measure of adequacy of iron availability n Monitor early response to iron therapy n Early diagnosis of iron deficiency in pediatric population n
- Slides: 54