A E R O M A P U





 syndrome: •")





- Slides: 34
A E R O M A P U N E R T I S R I A L S M IN I
Amenore a fisiologis : Keadaan prapubertas Hamil Menyusui Pasca menopause Amenorea patologis : Amenorea primer Amenorea sekunder
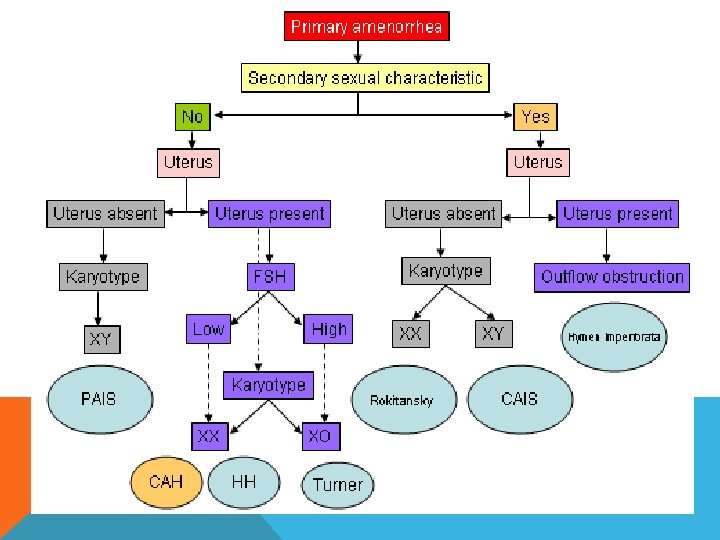
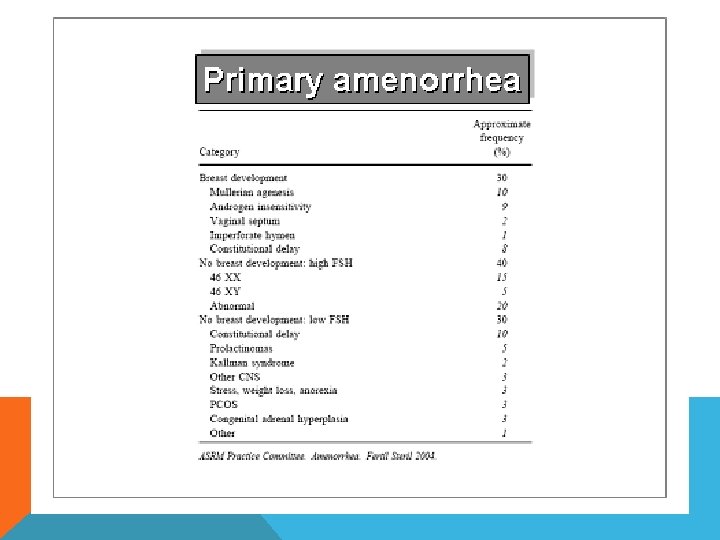
Amenorea Primer • Haid tidak terjadi bila wanita telah mencapai usia 14 tahun, pertumbuhan seksual sekunder belum terlihat • Haid tidak terjadi bila wanita telah mencapai usia 16 tahun, pertumbuhan seksual sekunder telah terlihat
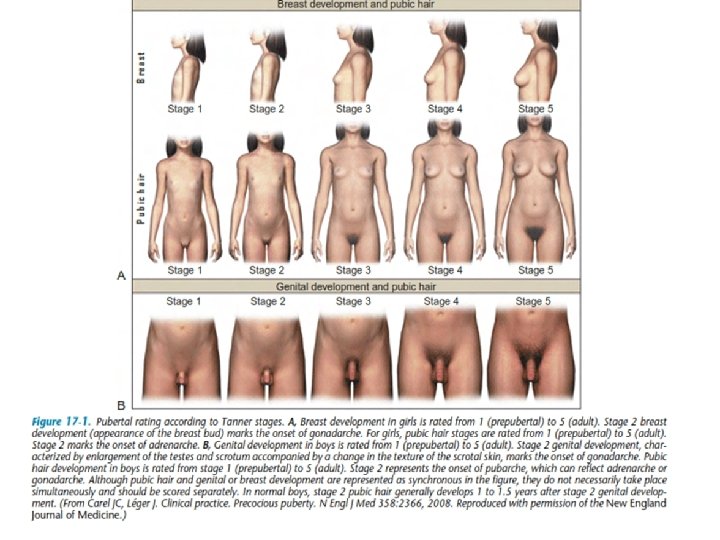
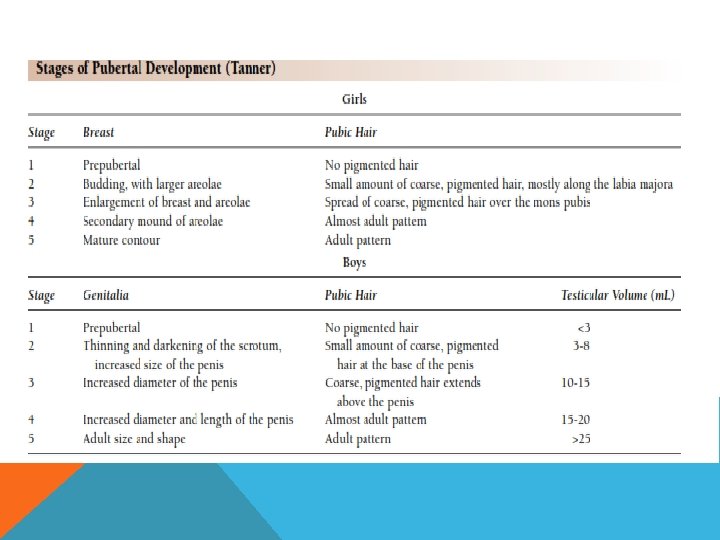
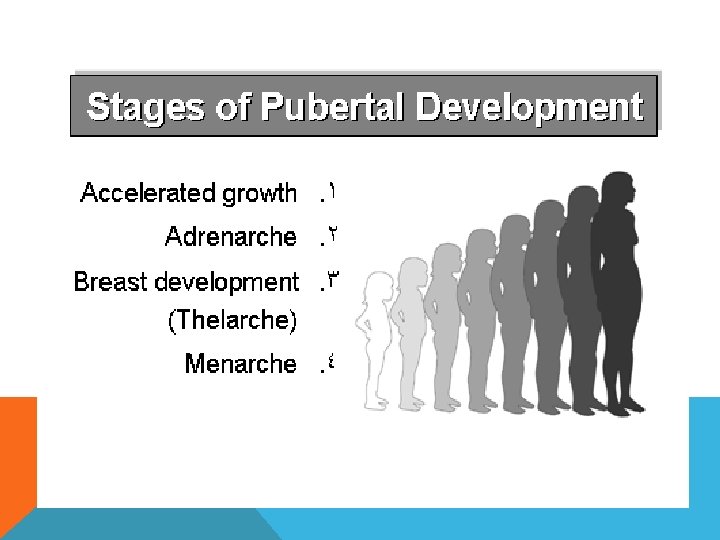
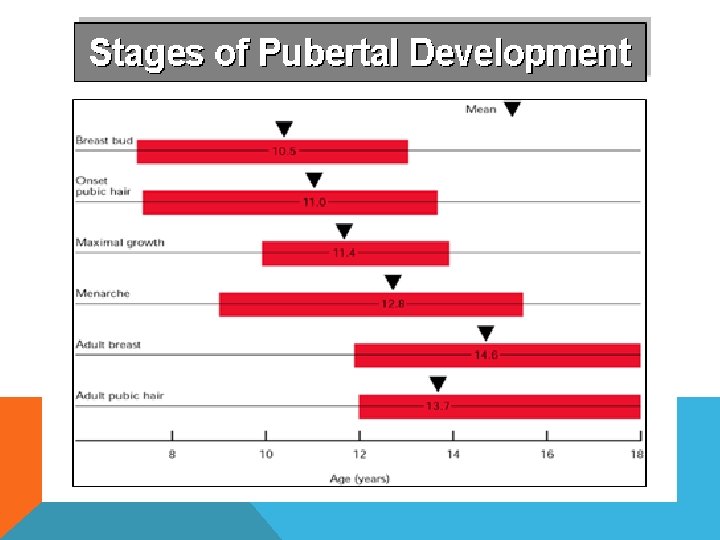
The first demonstrable sign of puberty in girls is breast development. Caution must be exercised in examination of breast tissue in obese girls, as simple fat may be mistaken for breast tissue. Pubic and axillary hair, acne, and body odour develop as a result of androgens secreted from the adrenal gland. The peak growth spurt occurs in Tanner stage 3 breast development, and menarche occurs in Tanner stage 4 breast development.
Mayer-Rokitansky Syndrome The following may be observed in patients with Mayer-Rokitansky-Kuster-Hauser (MRKH) syndrome: • Primary amenorrhea and possible cyclic abdominal pain • These symptoms are common in individuals with Mayer-Rokitansky. Kuster-Hauser syndrome. • The patient undergoes puberty with normal thelarche and adrenarche; however, menses do not begin. • Patients may report cyclic abdominal pain due to cyclic endometrial shedding without a patent drainage pathway. • Because ovarian function is normal, patients experience all bodily changes associated with menstruation and puberty.
Infertility Patients who do not undergo evaluation for primary amenorrhea often seek clinical attention for infertility. However, patients rarely proceed to infertility evaluation without ever having had a menses due to Mayer-Rokitansky-Kuster. Hauser syndrome. Although the ovaries function normally, the fallopian tubes may be closed, and the uterus is often anomalous. Inability to have intercourse The degree of vaginal aplasia can vary from complete absence to a blind pouch. The more shallow the canal, the greater the likelihood of the patient having dyspareunia. Renal malformations Absence or ectopia of the kidneys is common. Diagnosis can lead to discovery of renal anomalies. Some patients present with a history of voiding difficulties, urinary incontinence, or recurrent urinary tract infections (UTIs). Vertebral anomalies: Skeletal findings range in severity and clinical importance. Scoliosis is the most common of the skeletal anomalies.
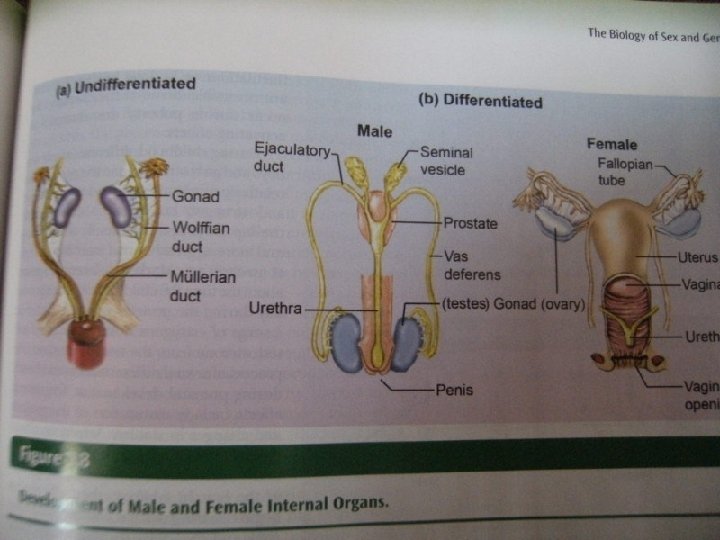
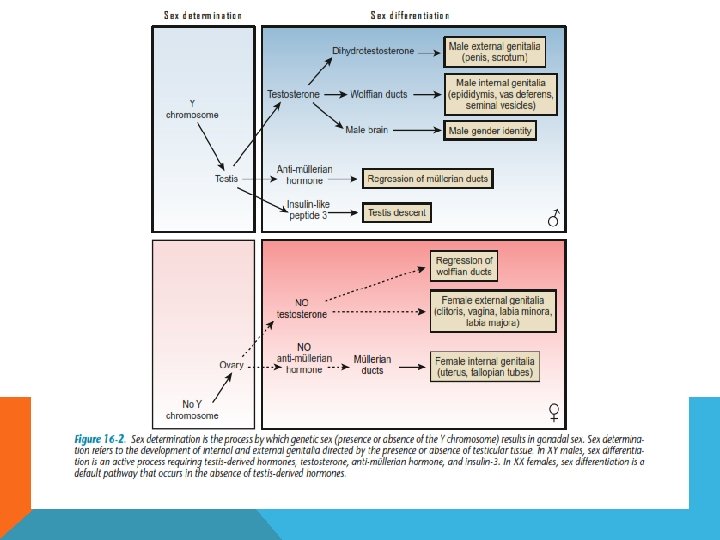
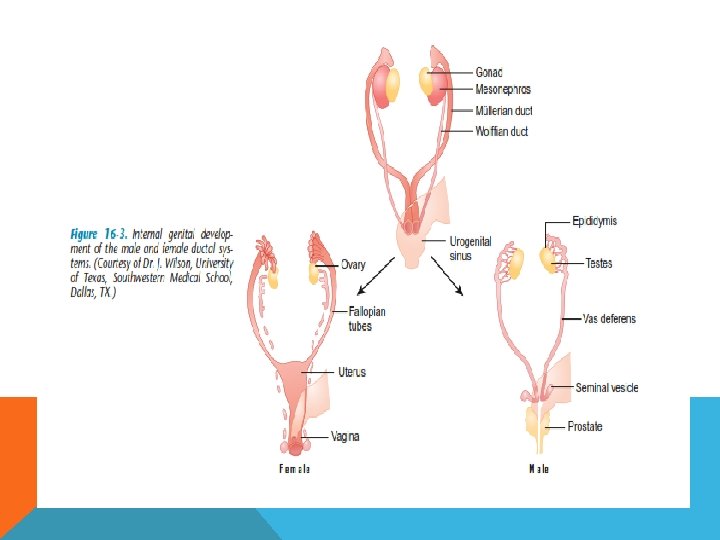
Normal secondary female sexual characteristics are present after puberty. Height is normal. Speculum examination of the vagina may be impossible or difficult because of the degree of vaginal agenesis. The vulva, labia majora, labia minora, and clitoris are normal. The cause of Mayer-Rokitansky-Kuster. Hauser syndrome is unknown, and no known gene is linked to this condition. A postulation is that the müllerian duct system ceases development during gestational days 44 -48. Although evaluation of patients with Mayer. Rokitansky-Kuster-Hauser (MRKH) syndrome can be performed on an outpatient basis, surgical repair requires admission. Medical and surgical care essential for capacity for sexual intercourse, and genital appearance. In rare cases, fertility may be possible. Using assisted reproductive techniques, women with Mayer-Rokitansky -Kuster-Hauser syndrome can become pregnant by having oocytes harvested, fertilized, and implanted in a surrogate.