A CASE OF NON ARTERITIC ISCHEMIC OPTIC NEUROPATHY

 residing in")









 Patient was found to have")











- Slides: 25
A CASE OF NON ARTERITIC ISCHEMIC OPTIC NEUROPATHY IN A YOUNG MALE Dr. Divya Motwani
48 years man worker at a construction site (operates with grinding machines) residing in Pune Chief Complaints - (RE) sudden, painless diminution of vision since morning
History Of Present Illness: Patient was apparently alright until he woke up in the morning and developed sudden, painless diminution of vision in the right eye since morning. Same sided headache since 2 days which was throbbing and continuous in nature. No history of flashes or floaters. No history of lifting any heavy weights. No history of spectacle use.
Past History : History of trauma to the right eye 15 years back with grinding particle while working after which the patient had mild watering and redness. No treatment was taken. No history of DM, HTN, IHD or any systemic illness. No history of any similar complaints in the past. Family History : not significant Personal History : Sleep , appetite , bowel , bladder was normal
General Examination: The patient was conscious , stable, well oriented to time place and person Systemic examination : WNL
OCULAR EXAMINATION OCCULAR EXAMINATION RIGHT EYE LEFT EYE VISION FC AT 2 FT , PL PRESENT, PR ACCURATE 6/12 P PIN HOLE NOT IMPROVING 6/6 P BCVA NOT IMPROVING 6/6 P (+0. 75 DS) EXTRA OCULAR MOVEMENTS FULL, FREE AND PAINLESS IN ALL GAZES HEAD POSTURE LID AND ADNEXA FULL, FREE AND PAINLESS IN ALL GAZES CENTRAL WNL
ANTERIOR SEGMENT EXAMINATION RIGHT EYE LEFT EYE CONJUCTIVA NORMAL CORNEA CLEAR ANTERIOR CHAMBER NORMAL DEPTH IRIS NORMAL PATTERN PUPIL C/C/RTL NO RAPD C/C/RTL LENS CLEAR IOP WITH APPLANATION TONOMETER 18 MMHG 20 MMHG
FUNDUS EXAMINATION RIGHT EYE LEFT EYE MEDIA CLEAR OPTIC DISC MARGINS BLURRED WNL CUP DISC RATIO NOT APPRECIATED 0. 2 NEURO RETINAL RIM NOT APPRECIATED HEALTHY MACULA NORMAL FOVEAL REFLEX PRESENT GENERAL FUNDUS TORTUOUS VESSELS WNL
RIGHT EYE
LEFT EYE
DIFFERENTIAL DIAGNOSIS Optic neuritis NAION AAION Impending CRVO
INVESTIGATIONS Routine blood reports – wnl (CBC, ESR, CRP) Patient was found to have raised homocystine levels – 39 mcmol/l (normal levels 4 – 15 mcmol/l) Colour vision test could not be performed due to poor vision. Perimetery could not be performed due to poor vision. OCT s/o mild edema of the optic disc in the right eye. Left eye optic disc –wnl
RIGHT EYE LEFT EYE
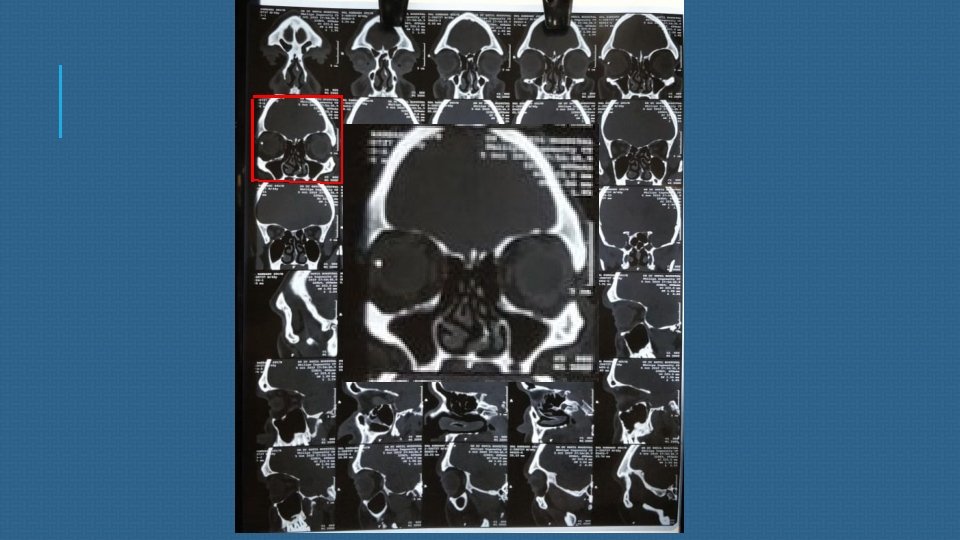
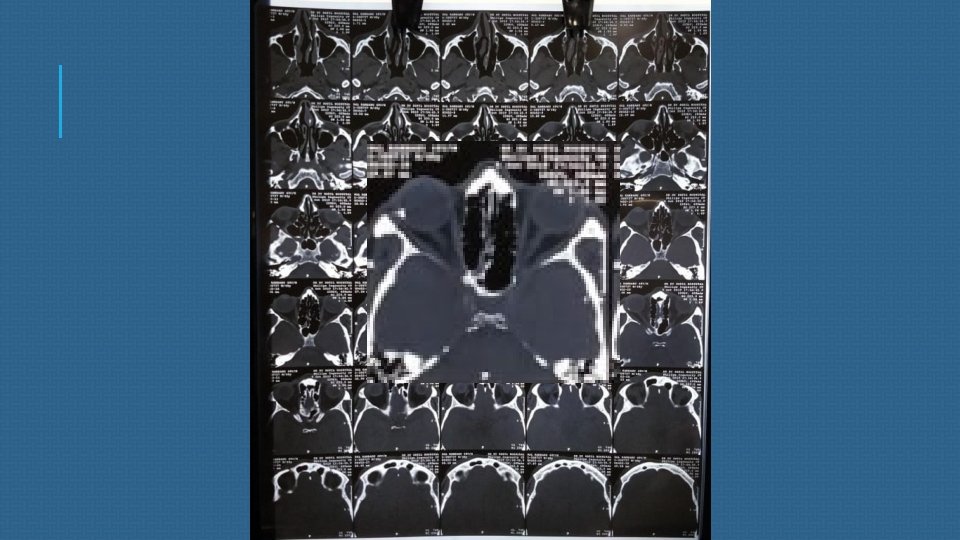
CT scan of brain and orbit S/o –a well defined metallic density, 10 x 4 mm along the lateral aspect of right eyeball/ deep to lateral rectus muscle within the right orbit s/o a foreign body.
YOUNG PATIENT HYPERMETROP IC DISC IN THE OTHER EYE SUDDEN DOV AFTER WAKING UP IN THE MORNING NO SYSTEMIC ILLNESS RE DISC WITH BLURRED MARIGINS
PROVISIONAL DIAGNOSIS RIGHT EYE NON–ARTERITIC ISCHEMIC OPTIC NEUROPATHY WITH INCIDENTAL INTRA OCULAR FORIGEN BODY.
PLAN OF MANAGEMENT v INJECTION IV METHYL PREDNISOLONE 1 GM/ DAY FOR 3 DAYS v. Followed by oral prednisolone 50 mg tapered every 3 days v (RE) E/D PREDISOLONE ACETATE 1% QID FOR 2 WEEKS v (RE) E/D NEPAFENAC 0. 1% TDS FOR 2 WEEKS v Folic acid supplements 5 mg for 1 month.
v. Takayama K, Kaneko H, Kachi S, Ra E, Ito Y, Terasaki H. High-dose intravenous pulse steroid therapy for optic disc swelling and subretinal fluid in non-arteritic anterior ischemic optic neuropathy. Nagoya J Med Sci. 2017; 79(1): 103– 108. doi: 10. 18999/nagjms. 79. 1. 103 v. Hayreh, Sohan Singh, and M. Bridget Zimmerman. “Non-Arteritic Anterior Ischemic Optic Neuropathy: Role of Systemic Corticosteroid Therapy. ” Graefe's Archive for Clinical and Experimental Ophthalmology, vol. 246, no. 7, 2008, pp. 1029– 1046. , doi: 10. 1007/s 00417 -008 -0805 -8.
ON FOLLOW UP The patient was symptomatically better after 1 week of treatment. The vision in the right improved to 2/60 NI on pinhole after 1 week. The disc edema reduced.
DISCUSSION Ischemic Optic Neuropathy is an acute, painless optic neuropathy occurring predominantly in patients over 50 years of age. AION is categorized as either arteritic or nonarteritic.
PATHOPHYSIOLOGY NAION Insufficiency of optic disc circulation d/t structural crowding of nerve fiber Inadequate oxygenation Ischemia and swelling of disc
TAKE HOME MESSAGE NAION IS ALSO AN IMPORTANT CAUSE OF SUDDEN LOSS OF VISION EVEN IN YOUNG PATIENT. A HYPERMETROPIC DISC IS AT RISK. HOMOCYSTINE LEVELS SHOULD ALSO BE EVALUATED IN SUCH INDIVIDUALS.
THANK YOU