A brief overview of CKD Harshani D Perera

A brief overview of CKD Harshani D. Perera Senior Registrar – Nephrology SJGH 09. 01. 2018

CKD – definition O Kidney damage or e. GFR < 60 ml/min/1. 73 m 2 persisting for 3 months despite the cause O several classifications O KDOQI – by National Kidney Foundation O KDIGO – by International Society of Nephrology
 guidelines , by")
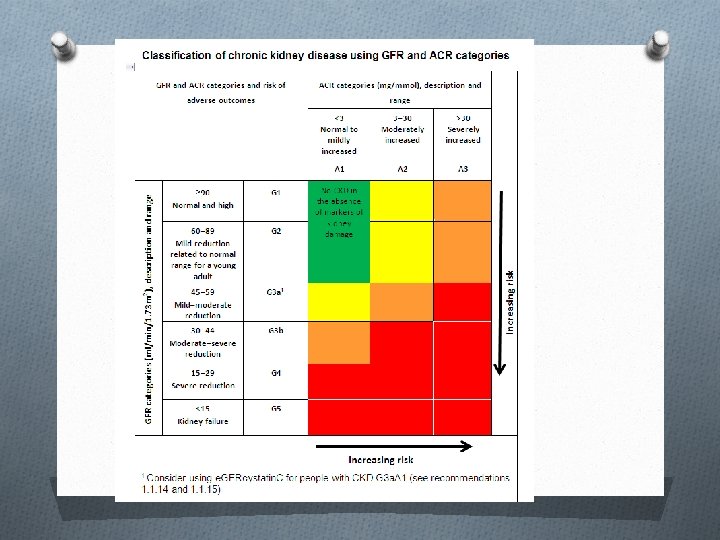
Classification - CKD O KDOQI (Kidney Disease Outcome Quality Initiative ) guidelines , by NFK O 5 stages of CKD O suffix T for patients with allografts O suffix D for patients on dialysis O 2012 KDIGO guidelines by ISN O 6 categories O G 1 to G 5 O G 3 – split in to 3 a, 3 b O A 1, A 2, A 3 – 3 levels of albuminuria
 : overall")
Calculating e. GFR O MDRD (modification of diet in renal disease formula) : overall MDRD more accurate O CKD-EPI Chronic kidney disease Epidemiology Collaboration) – O gender, race, age, Cr : are parameters need in both MDRD , CKD- EPI O Creatinine clearence : by Cockcrofr-Gault Equation : sex, age, weight, Cr, height (remains gold standard after 40 years) – less accurate than MDRD in obese and elderly

Limitations – classification CKD O Current CKD classification based on e. GFR O MDRD , CKD-EPI – both are relatively inaccurate in reflecting measured GRF above 60 ml/min O underestimate true GFR , thus over diagnose a large number of people having CKD stage 3 b O Physiological age related decline in kidney function in elderly – in absence of associated micro albuminuria seldom progress to ESRF

Progression of CKD O Current classification – not determined on progression of CKD O KDIGO – suggest , to define Progressive CKD ① sustained decline in e. GFR by 5 ml/min per year Or ② declining e. GFR category accompanied by 25% of drop in baseline e. GFR

Epidemiology - CKD O Prevalence 10% - 14% among general population O CAUSES : O Hereditary – APCKD O Acquired nephropathy : DM , HT, Glomerularnephritis, obstructive nephropathies

Rate of progression vary ! O According to underlying etiology. O Historically DM-nephropathy is the fastest , average decline around 10 ml/min per year. O In non diabetic CKD , chronic proteinuria GN having faster progression than low proteinuric CTIN-CKD. O In APCKD, beyond stage 3 b , more faster course. O Majority reach from stage 3 b to 5 progress to ESRF. O Some patients in CKD-5 remain stable for number of years.

Risk factors - CKD O Modifiable 1. Birth weight 2. Systemic HT 3. Diabetes 4. CVD 5. Albuminuria 6. Obesity / metabolic Xn 7. Dyslipidemia/smoking 8. Hyperuricaemia 9. Nephrotoxins – NSAID, herbal, Heavy metal O Non- modifiable Age (older) 2. Race (Non-caucasian) 3. Genetics 1.

Retarding progression of kidney disease ? O Typically natural progression does not proceed until nephron loss exceeds 50%. O Normal solitary kidney is vulnerable to natural progression if condition is congenital or acquired in early life. O LBW esp males progress to ESRF due to defective nephron development.

Proteinuria magnitude and risk of CKD progression O Magnitude of proteinuria is the strongest risk factor of CKD progression. O When it exceeds 500 mg/dl it co relate threshold of natural CKD progression. O Exception is highly selective albuminuria which can persists in nephrotic range even 10 years with out causing structural renal damage.

Non proteinuric CKD O CAUSES O Early phase of diabetic CKD O HT- GS O ADPCK O Chronic NSAIDs O Obstructive uropathy O Nephropathy of aging

Level 1 – kidney protective measures O Control blood pressure O ACEI or ARBS O avoid dihydropyridine unless needed for BP control O Control protein intake

Level 2 - recommendations O Restrict Na. Cl intake and diuretic therapy O NDHP –CCB O control each component of metabolic O O O syndrome Aldosterone antagonists Allopurinol therapy control serum PO 4 alkali therapy Bata blockers Avoid over anti-coagulation with warfarin

Functions of kidney O Fluid balance O Regulate electrolytes O Blood pressure regulation : RAAS O Ca / P 04 regulation- bone metabolism O Acid base balance O Endocrine function – erythropoietin / 1 OH CCF / Renin

Management of CKD O Early referral to nephrologist O Aim to slow down the progression : O Management of complications related to CKD O RRT counseling when CKD advances O when e. GFR – 20 ml/min O Refer to vascular surgeon for access creation if dialysis is decided. O Preserve non-dominant upperlimb for future AVF O Hepatitis B vaccination - dual doses 0, 1, 6 months

Preventing CKD progression O Most effective intervention is control of blood pressure : O HT is very common among in patients with CKD O Anti HT therapy O Life style modifications : O reduction of salt and alcohol O maintenance of healthy weight O regular exercise
 rise")
Anti hypertensive therapy O Fluid driven blood pressure (water and Na retention ) rise in advances CKD O Activated RAAS O usually multi drug regimens required. O ACEI and ARBS are first line in proteinuric CKD O risk of hyperkalemia especially during intercurrent illnesses O Choice of drugs depends on co-existing CVD, co-mobidities O Target : 130/80

Dietary advice O Obesity causes rapid progression of CKD, thus need weight loss. O Malnutrition common in CKD , it is multifactorial. O anorexia, acidosis, insulin resistance , inflammation , oxidative stress, urinary protein loss O low serum Albumin, Cholesterol, transferrin – are markers O Creatinine may stop rising due to reduction in muscle mass.

Recommendation - diet O Reduce protein intake slow the CKD progression – evidence based. O Protein energy malnutrition is common. O KDIGO – protein 0. 8 g/KBW/day when GFR < 30 ml/min O Avoid high protein intake >1. 3 g/KBW/d in patients at risk of CKD progression. O Salt restriction : < 5 g Na. Cl (90 mmol) per day. O In stage 4, 5 – restrict K , and PO 4.

Anemia in CKD O Common in stage 3 a and above O low Epo levels O reduced availability of iron O chronic inflammation O Monitor Hb levels annually till stage 3 a , then 6 monthly in advanced CKD.

Recommendation - anemia O Rule out other causes of anemia O Fe studies, blood picture, Vit B 12, foalte levels, stool occult blood, UGIE / LGIE O IV Iron : when T. Sat < 30 % O Correct deficiencies , if Hb still < 10 g/dl, start EAS ( Erythropoetin stimulating agents) If benefits overweigh potential harm – increased risk of stroke/thromboembolism, malignancies, hypertension

Benefits of anemia correction O Cardio- vascular benefits : regression of LVH, reduction of myocardial ischemia, reduced HR / CO O Increased quality of life : improved O exercise capacity, sleep patterns, immune functions, cognition, depression O Target Hb < 11. 5 g/dl should be maintained. O Hb > 11. 5 carry higher risk of cardiovascular events : stroke/ MI

Bone and mineral metabolism O Renal bone disease may already be manifested in CKD stage 3 b, and well established in ESRF. O Even it is well established patient may remain asymptomatic. O Active early management of CKD-BMD will prevent some of cardio-vascular complications.

Recommendations - BMD O check serum ionized Ca, PO 4 , intact PTH levels when e. GFR < 45 ml/min O optimal PTH target : 3 times upper range O correct hyperphosphatemia, hypocalcemia, and Vit D deficiency O Vit D suppliments / analogue O Phosphate binders O dietary phosphate restriction (dairy products, processed foods )

Complications of BMD O Coronary vessels calcification higher cardio-vascular risk O Heart valve calcification O soft tissue calcifications – calciphilaxis : indicating very poor prognosis in CKD. O Renal osteodystrophy

Metabolic acidosis in CKD O Failure of H+ excretion , may be compounded by accumulation of organic acids and bicarbonate loss in interstitial kidney diseases. O clinical manifestations rare till stage 5, dyspnoea occur due to respiratory compensation.

Metabolic acidosis … O aggravate hyperkalemia O inhibits protein anabolism O accelerate Ca loss from bone O correction of acidosis also slow the progression of kidney disease O KDIGO - recommends if HCO 3 < 22 mmol/L oral bicarbonate supplementations to maintain HCO 3 level above 22.

Cardiovascular risk O high prevalence of CVD among CKD patients. O most likely to die due to CV event than progress to ESRF. O KDIGO – recommends : level of coronary care should not be reduced by their CKD state. O Anti platelets in secondary prevention of CVD. O accelerate atherosclerosis : lipid lowering drugs for all above 50 yr, and young CKD patients with additional risk factors for dyslipidemia.

Risk of infection O Infection is second commonest cause of death in ESRF. O state of chronic immunosuppression , defect in both cellular and humoral immunity. O Annual influenza vaccine when e. GFR < 30 O Pneumococal vaccine for those who are high risk O Hepatitis vaccination : early as possible , preferably e. GFR > 30

Avoid risks of AKIs among CKD O All patients with CKD are at increased risk of O O O AKI Avoid nephrotoxins: NSAIDs, aminoglycosides, vancomycin , drugs causing interstitial nephritis Iodinating contrast for imaging better avoid unless benefits outweigh the risk of contrast AKI. poor renal perfusion : volume depletion , over diuresis , diarrhoea, vomiting sepsis heart failure , MI, tachyarrythmias

Increased bleeding risk O Uremic platelet dysfunction O mild to moderate thrombocytopenia is commonly seen among ESRF O Inadequate dialysis O anemia O Heparin use for dialysis Options : adequate hemodialysis, correction of anemia, platelet transfusion, cryopercipitate, desmopressin nasal spray, tranexamic acid

Timing and initiation of RRT O All patients with e. GFR < 20 , or who are likely O O to progress to ESRF in 12 months should receive education and counseling to aid their decision on best RRT modality. If HD is preferred AVF referrel If PD is preferred CAPD catheter insertion 3 weeks prior. Kidney transplant : Pre-emptive is the best , offer when e. GFR <20 , before dialysis. explore the possibility of live donor if KT opted.

“Conservative” Management O Potential burden of commencing RRT in terms of O O O high short term mortality rates Recurent hospitalizations Time spent for travelling Limited improvement of quality of life Multiple co-morbidities Advanced malignancy O Offer active medical management and follow up with out starting dialysis. O distressful advanced uremic symptoms – need palliative care to facilitate suffering free death.

Conclusion O Rising global trend of CKD during last few O O O decades. Diagnosis of CKD is challenging and by exclusion of AKI when there is no baseline Cr available. CKD management guidelines are freely available which is helpful to provide standards of care. Asses the progression of CKD Delay the progression of CKD while managing CKD related complication. Early referral to nephrologist and on time RRT counseling are key in successful management.

Thank You.
- Slides: 37