672021 SKELETAL Tuberculosis Potts disease tuberculous spondylitis Infectious

6/7/2021

SKELETAL Tuberculosis

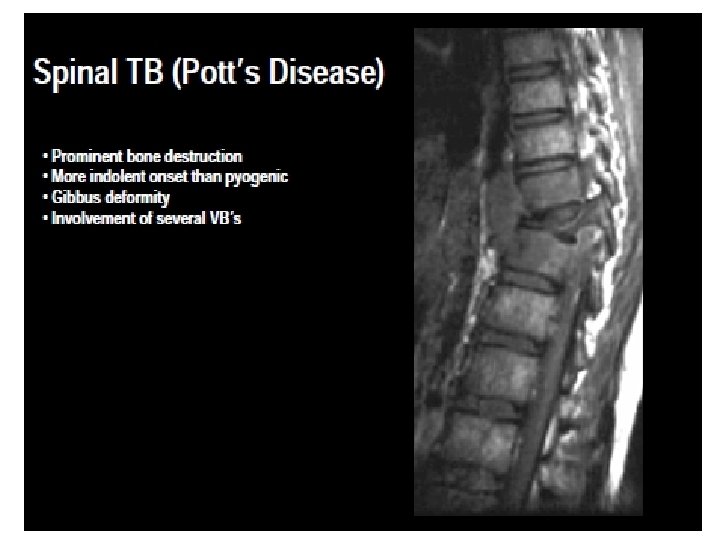
Pott’s disease - tuberculous spondylitis

Infectious spondylitis • Infection by a specific organism of one or more components of the spine, namely the vertebra, IV discs, paraspinal soft tissues, and epidural space • Pyogenic spondylitis – Post-operative infection – Hematogeneous • Granulomatous spondylitis – TB spondylitis – Fungal spondylitis

Epidemiology TB SPONDYLITIS • • • 60% of skeletal TB Sex: Equal Age: Mostly ˂30 Y No age immune Spine : commonest site of skeletal TB d. t high blood flow Site: Lower dorsal>lumbar>upper dorsal>cervical • Spinal TB + pulmonary TB in ⅓: ⅔ of cases. • Develops insidiously→ gap of several months between onset of symptoms and diagnosis

Sources q Hematogeneous dissemination of tubercle bacilli from a primary or reactivated focus. ARTERIAL? q Extension from a paraspinal infection -Rare. atlantoaxial TB: Contiguous spread from an apical pulmonary focus of active TB q Lymphatic drainage from an adjacent affected area such as the pleura or a kidney -Rare
 near upper or lower surface")
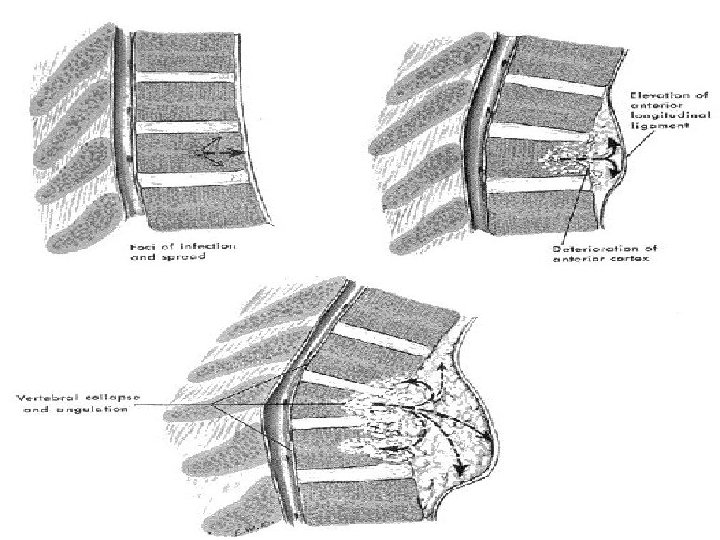
Site of initial lesion 1. • Paradiscal 50% (Metaphyseal) near upper or lower surface 2. • Anterior (Subperiosteal) 3. • Central 4. • Appendiceal • Usually affect 2 vertebrae or more, multiple affection 50% • Skip lesion : 2 unrelated foci at different level • Local changes: • Body: destroyed-replaced by necrotic caseous material→ collapse • Disc: late affection-sequestrated -may extrude post. → paraplegia • Spread of infection Along ALL→ Paravertebral abscess

Two distinct patterns : • classic finding →destruction of 2 or more adjacent vertebrae and opposed end plates, disc infection, and commonly a paraspinal mass or collection; • Atypical form →without disc involvement is the second pattern(more increasing)

Pathogenesis & Pathology • Granuloma→ bone expansion→ destruction →in a later stage, cartilage destruction →adjacent disc space involvement (late: avascular)→disc interval collapse →kyphosis & Gibbus • No bone regeneration or periosteal reaction • If only one vertebra is affected, the disc is normal, but if two are involved the intervertebral disc, which is avascular, cannot receive nutrients →collapses. • A dry soft tissue mass often forms and superinfection is rare.

SIGNS AND SYMPTOMS • GENERAL • Constitutional symptoms such as low-grade fever with evening rise, lethargy, malaise, night sweats, anorexia and weight loss are not as common as in pulmonary TB

LOCAL • Pain: localized dull ache, worse after standing, walking • Tenderness : localized over spinous processes • Stiffness & limited spine movement d. t. spasm of erector spinae • Deformity: Angular kyphosis • Cold abscess • Neurological deficit : Radicular pain, severe cauda equina syndrome, and paraplegia Classic triad: Back pain, fever, and neurological deficits found in only 15% patients

Diagnostic tests • CBC -anemia, hypoproteinemia -normal WBC, normal ESR in up to 10% of the cases - ↑ ESR does not advance the diagnosis, for follow up • Tuberculin skin test when positive is not of much help either especially in endemic areas or with recipients of BCG vaccine • may be negative in as many as 20% of the patients with vertebral TB.

The physical appearance – Potts disease of spine - gibbus

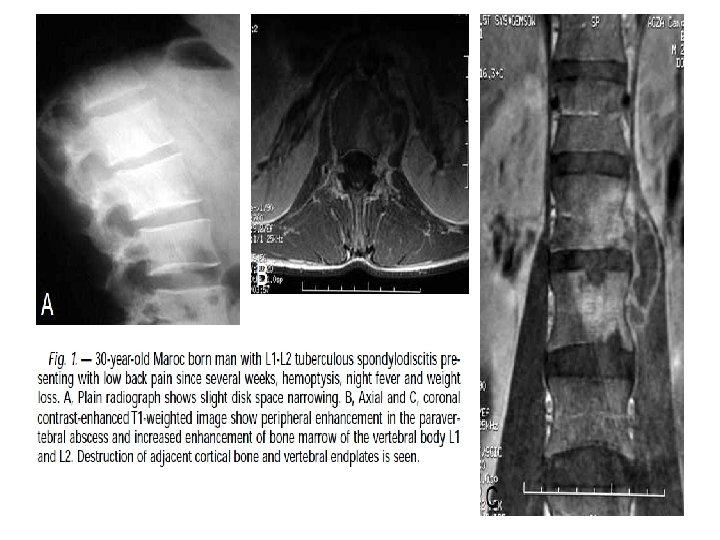
X- RAY • • 2 or more adjacent vertebrae: multilevel- multicenteric Lost height + erosion of end plate Rarefaction→ destruction → collapse Disc space narrowing Paravertebral mass + soft tissue calcification No new bone formation DISADV. : • insensitive for the early detection of vertebral TB. • vertebral involvement is not detected until at least 50% of the trabecular bone is lost • of limited value in evaluation of the posterior arch, particularly in the thoracic spine • no specific or pathognomonic findings distinguish TB from pyogenic spinal infection

Demonstrates involvement of three vertebrae anteriorly, and the bodies of L 2 and L 3 have collapsed and become fused

TB Spine X ray • loss of vertebral body height • sclerosis of the end plates, and anterior scalloping

Pyogenic spondylitis Disc space narrowing Loss of Vertebral endplate cortex Vertebral collapse Paraspinal soft tissue infiltration. Abscess formation – 2 adjacent vertebrae with disc – – – Location: L (48%)>T(35%)>C(6. 5%) TB spondylitis – End plate irregularity with vertebral body destruction and sclerosis – Multiple non(contiguous) vertebral involvement – Large paraspinal abscess – Calcification over chronic paraspinal abscess – Isolated posterior involvement possible – Middle T> T-L junction>L and C

Imaging Features that Favor Spinal TB Rather than Neoplastic Disease

C. T. • Detect small, early foci of bone infection and the extension of the bone and soft tissue involvement • End plate destruction, fragmentation of the vertebrae, and paravertebral calcifications are adequately demonstrated. • CT-guided fine needle aspiration has become widely accepted for both culture and histological diagnosis.

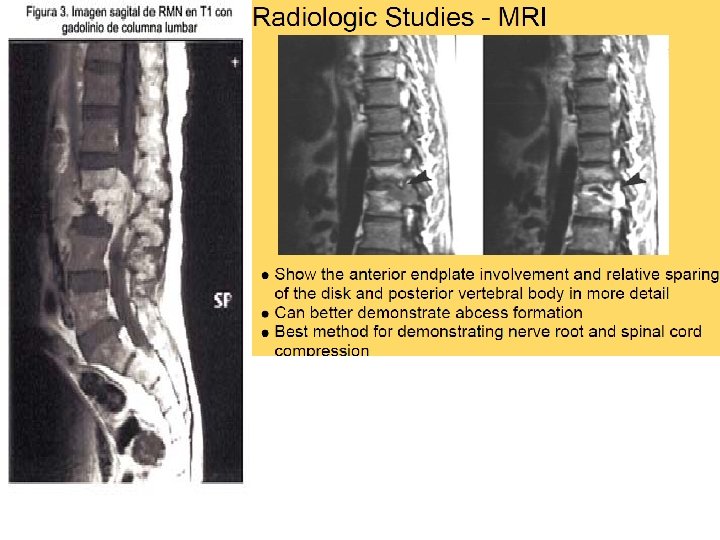
MRI • first choice in the evaluation and follow-up of spondylodiscitis. q Higher sensitivity for detection of early inflammatory BM changes and infiltrative end plate changes in the vertebra q Bone fragments q Show paravertebral, epidural, and intraosseous abscesses q Extent of cord compression q Presence of intramedullary lesions. q high signal of intervertebral disc on T 2 W. Bone- soft tissues- cord

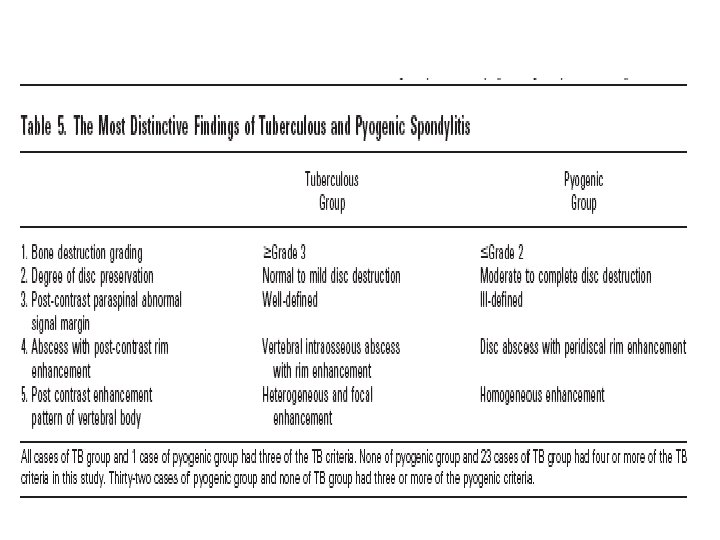
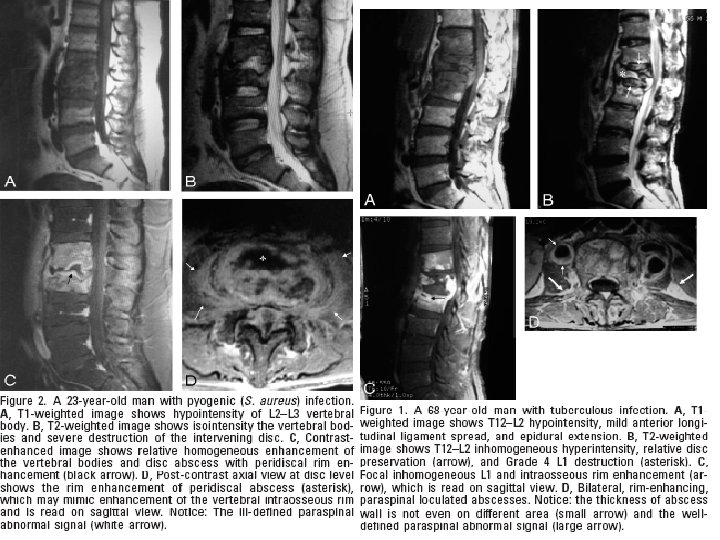
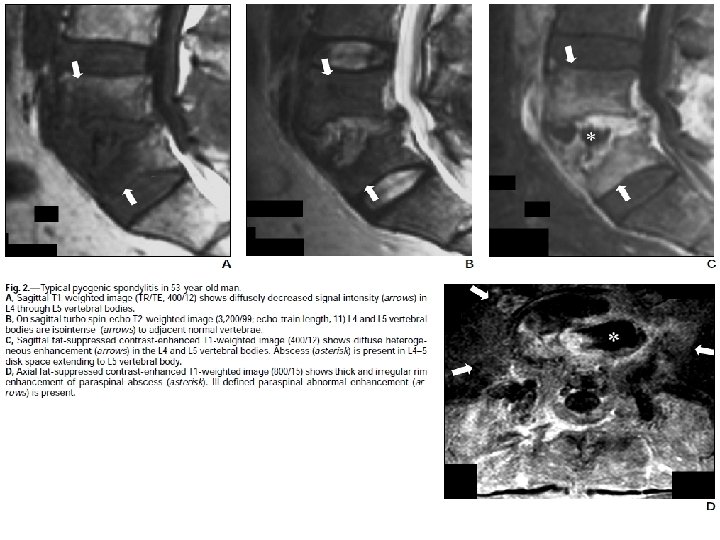
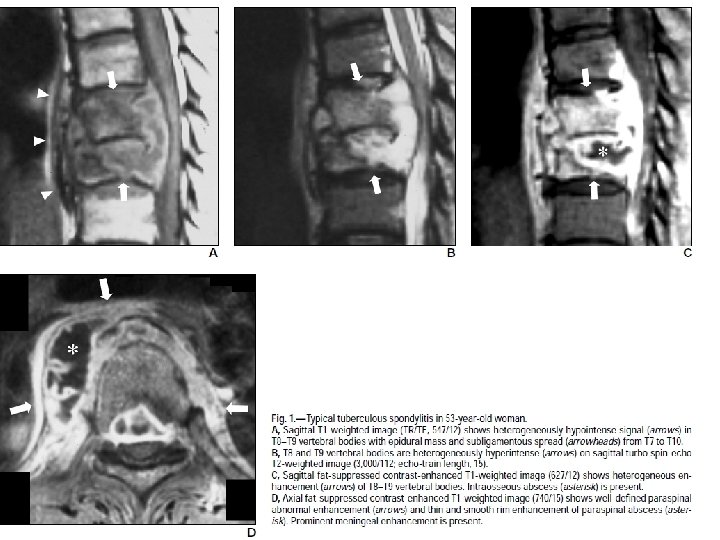
MRI pyogenic spondylitis – Disc abscess with peridiscal rim enhancement – Disc destruction>bone destruction – VB enhancement: Diffuse and Homogenous – Ill-defined paraspinal signal – Low kyphotic angle change in Xray and MRI TB spondylitis – Bone destruction> disc destruction – VB enhancement: focal and heterogenous – Epidural extension – ALL spread – Paraspinal calcification – Pedicle destruction – vertebral intraosseous abscess with rim enhancement


DD of vertebral tuberculosis • Low-grade pyogenic infections, such as brucellosis, and other bacterial and fungal infections. • Granulomatous diseases (sarcoidosis), • Traumatic and osteoporotic fractures, • Primary and metastatic neoplasms • Bone deformities such as Scheuermann disease.

D. D q Tuberculosis →if a large, calcified paravertebral mass and absence of sclerosis or new bone formation q Reduced height of an intervertebral disc is only rarely seen in neoplastic forms, q Pyogenic spondylodiscitis : rapid loss of height in the disc with destruction, along with extensive sclerosis, the absence of gibbus deformities and the absence of calcified paravertebral masses. q Brucellar spondylitis include gas within the disc, a minimal associated paraspinal mass, absence of kyphosis and a predilection for the lower lumbar spine.

TB vs. Pyogenic

COMPLICATIONS • • Vertebral collapse resulting in kyphosis Spinal cord compression sinus formation paraplegia (so called Pott's paraplegia)

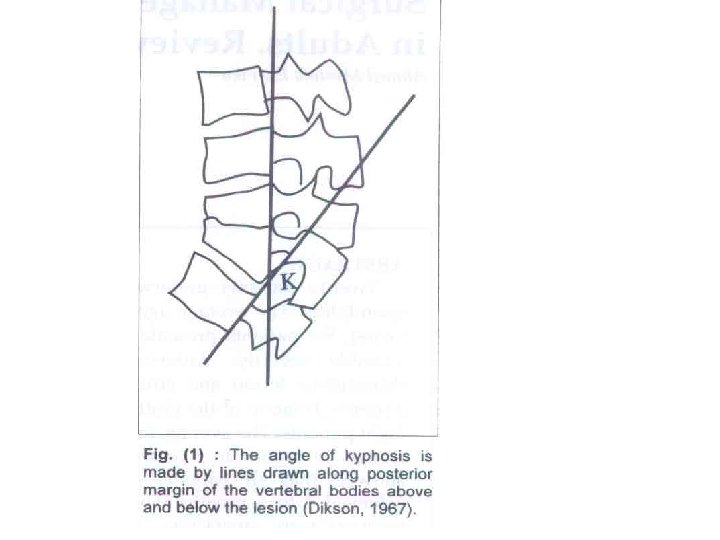
1. ANGULAR DEFORMITY • Collapse is limited to front of the bodies as the post part is held by the unaffected neural arch • Apex of deformity : Gibbus • In Thoracic spine: Kyphosis • In lumbar &Cx (normally lordotic) : Flattening
, q. Thoracic involvement, q. Multiple levels of involvement, q")
Risk factors q. Age (children), q. Thoracic involvement, q. Multiple levels of involvement, q Greater initial loss of vertebral height. q. Radiographic “at risk” factors : include dislocation of the facets, retropulsion of diseased fragments, lateral translation of a vertebra

2 - COLD ABSCESS • Def: Tuberculous collection of caseous material , pus, disintegrating bone & debris • Occur in 70% of pt. with spinal TB • Slow formation, last for years with no tendency towards healing; a chronic abscess. • Slow development, that there is little inflammation and it becomes painful only when there is pressure on the surrounding area. • Site, anywhere, but it is most commonly found on the spine, hips, lymph nodes or in the genital region.

SITE • 1 st it is a paraspinal abscess –along ant. Border of vertebra under ALL • Then: Remain so Trickle along fascial &anatomical planes q. Dorsal TB: Extend - posterior mediastinal mass - Retrophrenic abscess -Mass in back q. Lumbar TB: Psoas abscess point post in lumbar ∆ Trickle in buttock…proximal thigh q. Cx TB : Retropharyngeal—post neck ∆- mediastinum

3 - Pott’s paraplegia • In 10% of Pott’s • Occur mostly in Thoracic TB –narrow canal -commoner • In the lumbosacral region up to three-quarters of the spinal canal may be compromised before the patient develops neurological symptoms. • The margin of safety is much less in cervical and thoracic spinal canals

• The first classification was made by Sorrel and Dejerine in 1924. Paraplegia was divided into two groups as early onset and late onset. • Hodgson et al described two basic groups in preoperative evaluation of the lesion. q Group A: paraplegia with active disease, which included two subtypes: (1) external pressure on the cord; (2) penetration of the dura by infection; q Group B: paraplegia of healed disease, which included two subtypes: (1) transection of the cord by a bony ridge; (2) constriction of the cord by granulation and fibrous tissue.

EARLY ONSET PARAPLEGIA • Type A : arise while dis. Is active-1 st 2 years Paraplegia w arise , progress, subside parallel to d* activity -causes: Inflammatorypressure of cold abscess or cord congestion & edema -Spontaneous recovery may occur -Need simple abscess evacuation • Type B : Paraplegia w NOT subside as d become quiescent -cause: Mechanical cord pressure by seq. bone-disc-bony ridge -No recovery unless decompression • Type c : Sudden onset paraplegia -Causes: Thrombosis of cord vessels-Need decompression • Type D : collapse w out angulation Progressive paraplegia w simulate tumour -causes: TB lamina--- Encysted TB of back of vertebra -Need laminectomy

LATE ONSET PARAPLEGIA arise after apparent disease arrest >2 y Type A: Incomplete healing Reactivation occur after apparent cure≥ 2 Y cord is compressed by inflamm. Material Type B : Insidious onset paralysis occur many years after quiescent d Causes: Longitudinal cord shrinkage d. t. prolonged friction &dragging of cord against angled kyphosis→ irreversible impairment of long tract conduction Late-onset paraplegia may be seen when the tuberculous spine heals with a kyphosis of 60° or more, and in children if the kyphosis progresses with growth Underlying pathology is tuberculous caseous tissue, tuberculous debris, sequestra of vertebral body, internal gibbus, and deformity

Clinical features Symptoms and signs • The onset is insidious manifesting itself either by motor weakness or sensory impairment in lower limbs, or dysfunction of bladder or bowel. • Clumsiness, incoordination, weakness are early symptoms, voluntary movement ability decreased, muscle tone increased and tendon reflexes brisk. • Clonus and extensor plantar reaction, • paraesthesia or numbness may occur. poor prognosis is encountered in patients with a complete paraplegia, flaccid paralysis, rapid development, longer duration of symptoms >6 M , and late onset of disease (“healed disease”).

m

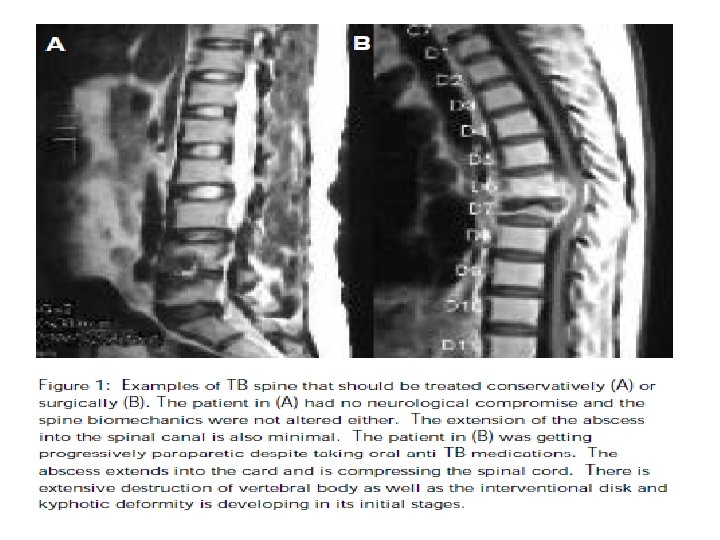
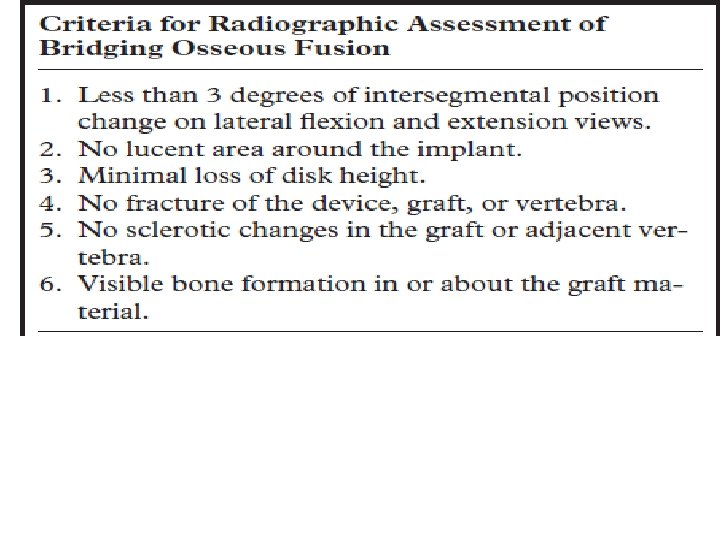
Management of TB spondylitis – The aim of treatment in spinal tuberculosis is to Eradicate the disease ; and to Arrest and correct any kyphosis – Anti-TB medication vs. Anterior debridement with interbody fusion

Surgical plan • Golden standard: anterior debridement with interbody fusion • Instrumentation – Anterior or posterior ( 1 stage or 2 stage) – Level • Graft – Autogenous: Iliac bone, fibular, rib – Allogenous – Titanium cage

Indications q. Advanced paraparesis at presentation, especially in a young patient, q. Kyphotic deformity, either progressive or established. This is most commonly seen in the cervical and dorsal spine q. Late -onset paraplegia and pseudo-arthrosis in healed tuberculosis may require decompression and correction of deformity by instrumentation. q. Intractable pain due to presence of epidural mass compressing theca and nerve roots, along with spinal instability qlarge palpable cold abscesses in the neck and groin. need to be drained. This reduces pain and conservative management becomes more effective as bulk of the disease is reduced Early operative treatment with instrumentation, when indicated, combined with chemotherapy, minimizes neurological deterioration and spinal deformity, allows early ambulation, and results in excel lent neurological recovery

qclinical factors (neural arch involvement, recurrent paraplegia, and massive retropharyngeal abscess causing difficulties with ventilation or swallowing), qtreatment factors (persistant or progressive deficit while following an adequate course of conservative treatment), qimaging factors including panvertebral involvement [scoliosis or severe kyphosis on plain films, global destruction on (CT) or MRI or extradural compression (circumferential cord compression from granulation tissue on MRI), qpatient factors (painful spasm or nerve root compression).
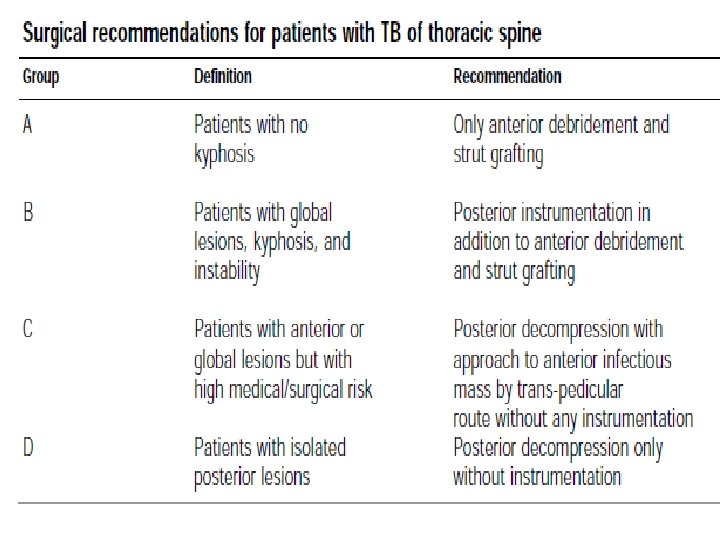

• Since tuberculosis affects principally the vertebral bodies, ant. decompression is usually recommended • Concomitant posterior instrumentation is indicated to 1 -neutralize gross instability from panvertebral disease, 2 - to protect the anterior bone graft, 3 -to prevent graft-relate complications after anterior decompression in long segment disease, 4 - to correct kyphosis • If posterior stabilization is undertaken without previous anterior decompression the kyphosis cannot be corrected. • If anterior decompression and fusion are performed first without instrumentation, the spine is rendered grossly unstable increasing the risk of further neurological injury until secondstage instrumentation is undertaken

• The ideal procedure would allow an anterior decompression and fusion, posterior instrumentation with or without posterior-column shortening and fusion to be carried out in one stage through a single approach • The indications for correction of the kyphus : -An adult with loss of more than one and a half vertebral bodies loss with an anticipated final kyphosis angle of 60° or more -More than two radiological signs of progressive kyphosis

• The vertebral column is at its weakest immediately after debridement and bone grafting. The graft is able to provide sufficient stability and structural support in only 41% of patients with a short defect. • Graft > 4 cm: 5 cm long, needs to be protected to prevent graftrelated complications such as fracture, or displacement with a consequent increase in kyphosis and/or increase in the neural deficit • Stabilization of the spine is indicated if there is a panvertebral lesion, if the post-debridement defect spans more than two discs (5 cm or more) or when correction of the kyphus is contemplated • The advantage of posterior instrumentation -Good fixation can be achieved in healthy posterior vertebra -Instrumentation only needs to extend one healthy segment above and one below

• The ideal procedure is a single-stage anterior decompression followed by posterior instrumented stabilisation and anterior grafting • Transpedicular decompression and instrumentation objective was not to correct a kyphosis but to prevent its progression and hence surgery was only carried out over one or two levels • the first successful fusion procedures were described by Hibbs and Albee in 1911 for prevention of progressive deformity from Pott’s disease

6/7/2021
- Slides: 58