5 Diabetes Mellitus Chronic complications Treatment Diabetic macroangiopathy

Лекция 5 Diabetes Mellitus: Chronic complications, Treatment


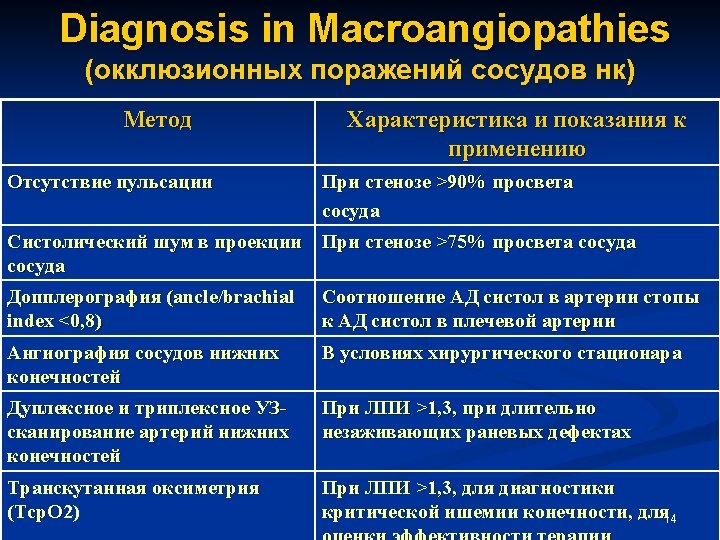
Diabetic macroangiopathy 1. Ichemic heart disease and heart failure (painless IHD, the same frequency in mails and femails, high risk of sudden cardiac death, high frequency of complications in myocardiac infarction) 2. Cerebrovascular diseases (stroke, functional apoplexy, demention) 3. Periferial angiopathy (occlusion of periferial arteries of lower limbs) Types of occlusion -pelvic (aorta, ileac arteries) -femoral (femoral, popliteal arteries) -periferial (leg and foot arteries) Stages I stage – nonsymptomatic (absence of pain) II stage – pain in physical exercises (“intermittent claudication”) III stage – pain in rest (costant form) 3 IV stage – trophic disorders (necrosis, gangrene)


Stratification of risk for CVD in DM Risk factor Уровень АД (мм рт. ст. ) 120 -129/8084 130 -139/9099 140 -150/90 - 160 -179/100 99 (1 ст. ) -109 (2 ст. ) ≥ 180/110 (3 ст. ) No RF Non significant risk Low Moderate High 1 -2 RF Low Moderate High Very High 5
")
Stratification of risk for CVD in DM RF Уровень АД (мм рт. ст. ) 120 -129/8084 130 -139/9099 140 -150/90 - 160 -179/100 99 (1 ст. ) -109 (2 ст. ) ≥ 180/110 (3 ст. ) ≥ 3 RF or Presence of DM or injury of target organs Moderate High Very High Associated to DM Clinical states Высокий риск Очень высокий риск 6

 ypes of occlusion")
Diabetic macroangiopathy eriferial angiopathy (occlusion of periferial arteries of lower limbs) ypes of occlusion pelvic (aorta, ileac arteries) emoral (femoral, popliteal arteries) periferial (leg and foot arteries) tages (классификация Фонтейна- Покровского) stage – nonsymptomatic (absence of pain) stage – pain in physical exercises (“intermittent claudication”) I stage – pain in rest (costant form) V stage – trophic disorders (necrosis, gangrene) Особенность при СД: Болевой синдром может отсутствовать Трофические нарушения могут возникать на любой стадии 9





Treatment of chronic Complications
 2. Lazerphotocoagulation (local,")
Treatment of rethinopathy Compensation of carbohydrate metabolism (Hb. A 1 c<7%) 2. Lazerphotocoagulation (local, panrethinal) 3. Vitreoectomy with endolazercoagulation Indication for lazercoagulation: - dilatation of cappilaries and significant convolution of small vessels in paramacular zone, evidence of solid exudates, rethinal edema, maculopathy - multiply rethinal hemorragies, microaneurisms in paramacular zone and other sites, convolution of vessels, irregular dilatation of veins, soft exudates - growth of new vessels, fibrosis, rethinal and prerethinal hemorragies 17
 и")
Treatment of rethinopathy При исходно выраженной декомпенсации (Hb. A 1 c > 10%) и ПДР надо начинать с LFC, т. к. быстрое улучшение углеводного обмена – прогрессирование ДР и ухудшение зрения. - Снижение гликемии у таких больных надо проводить очень медленно после ЛКС. Indications for cryocoagulation n Rubeosis glaucoma n Anterior proliferation of rethinal vessels (in iris area, eye lens, angle of anterior bulbi camera) Indications for vitreoectomy n Big vitreal hemorrage with slow resorption (over 4 -6 months) n Traction of rethina 18 n Old fibrosis changes in vitreal body -
 n")
Treatment of diabetic nephropathy Microalbuminuria stage n Compensation ofcarbohydrate metabolism(Hb. A 1 c<7%) n ATE inhibitors and ARA in supressive dasages in normal level of AP and in therapeutic dosagesin AP>130/80 mm p. m. n Glycosaminoglicans (sulodexid) – 2 courses/year n Correction of dislipidemia Diet with moderate reduction of animal‘s protein not over 1 g/kg BM Proteinuria stage n Compensation ofcarbohydrate metabolism(Hb. A 1 c<7%) n ATE inhibitors and ARA to support AP (130/80) n Glycosaminoglicans (sulodexid) – 2 courses/year n Correction of dislipidemia n Reduction of animal‘s protein in diet till 0, 8 g/kg BM n Erythropoetin in renal anemia 19
 n n n Compensation of")
Treatment of diabetic nephropathy Stage of chronic renalfailure (CRF) n n n Compensation of carbohydrate metabolism(Hb. A 1 c<7%) ATE inhibitors and ARA to support AP (130/80) Correction of dislipidemia Reduction of animal‘s protein in diet till 0, 8 g/kg BM Erythropoetin in renal anemia (Hb<110 g/l) Correction of increased potassium level Correction of phosphor-calcium metabolism Enterosorbtion Terminal stage Hemodialyses Peritoneal dialysis Renal transplantation 20

Treatment of diabetic neuropathy n n n n Treatment of Diabetic Polyneuropathy Compensation of carbohydrate metabolism(Hb. A 1 c<7%) Thyoctacid drugs (600 mg with 200 ml of physical solution intravenous infusion N 15, then per os 300 mg/2 times daily till 1 -2 mnths, two courses/year Vitamines B-group (100 -300 mkg 1 -3 times daily 3 mnths, two courses/year Anticonvulsive drugs (200 -600 mg x 1 -3 times daily – constant treatment) Tricyclic antidepressants 5 -25 mg x 1 -3 times daily Symtomatic treatment of pain and convulsions(nonsteroid untiinflammatory drugs) Polyvitamines and polimineral complex drugs(1 mnth)< 2 -3 courses/year Treatment of Diabetic Autonomic Neuropathy Compensation of carbohydrate 21 metabolism(Hb. A 1 c<7%)

Treatment of diabetic foot syndrom n n n n Treatment of neuropathic foot syndrom with preulceration and evident ulceration Compensation of carbohydrate metabolism(Hb. A 1 c<7%) Removing of skeen sites with hyperkeratosis and primary debridiment Antibiothic therapy in skeen defect infection of 2 -nd stage and deeper Using of atraumatic bandage Treatment of neuropathic foot syndrom with osteoarthropathy Compensation of carbohydrate metabolism(Hb. A 1 c<7%) Using of atraumatic bandage Biphosphonates (pamidron acid 90 mg intravenous infusion, aledron acid 10 mg/sec, ethidron acid 20 22


Treatment of diabetic foot syndrom Treatment of ichemic form of diabetic foot 1. Concervative treatment: n Compensation of carbohydrate metabolism(Hb. A 1 c<7%) n Stop smoking n Correction of AP n Treatment of dislipidemia n To breake ichemia of extremity (desaggregants; antycoagulants; prostaglandine E drugs 920 -60 mg intravenous infusion with 250 -400 ml of physical solution n 20 -30, 2 -3 courses/year) 2. Restitutive surgery of arteries and/or transcutaneous ballon angioplastic 3. Using of antibiotics in injuring of extremity 24

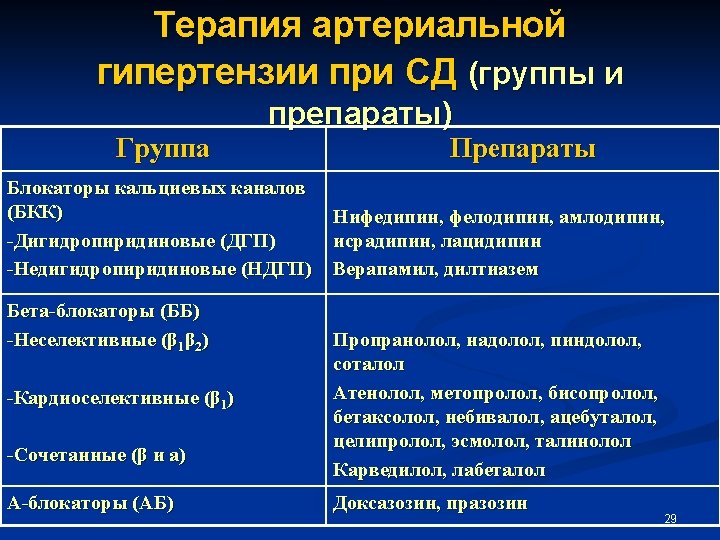
Treatment of Diabetic Macroangiopathy Ichemic heart disease 1. Concervative treatment: n Compensation of carbohydrate metabolism(Hb. A 1 c<7%) n Stop smoking n Correction of AP (ATE inhibitors and ARA, diuretics, β-blockers, α-blockers, Ca-channel antagonists, druga of central action) n Treatment of dislipidemia (statines, sequestrators of biliar acids, fibrates) n Analgesic drugs (nitrates, β-blockers, Ca-channel antagonists) n Asperine (75 -300 mg/daily) 25 2. Surgical treatment
 n")
Treatment of Diabetic Macroangiopathy Hart failure 1. Concervative treatment: n Diuretics (potassium saving) n ATE inhibitors n β-blockers n Cardiac glycosides n Inotropic drugs 2. Surgical treatment (heart transplantation) Treatment of macroangiopathy of lower limbs 1. Conservative: n Aspirine “cardio” (100 -300 mg) n Prostaglandine E drugs n Anticoagulants n Hypolipidemic drugs 2. Surgical: n Revascularisation n Amputation 26





THANK YOU FOR ATTENTION ! 32
- Slides: 32