46 xx DSD Dr Hashemi Pediatric Endocrinologist Assistant























 11 Hydroxylase")














- Slides: 60
46, xx DSD Dr. Hashemi Pediatric Endocrinologist Assistant Prof. of Shahrekord University Of Medical Sciences 1
Normal Sex Development The distinction between male and female is considered absolute so that sex assignment at birth is instantaneous. 2
Normal Sex Development ü Chromosomal sex ü Gonadal sex ü Phenotypic sex ü Brain sex 3
Chromosomal sex v Chromosomal sex refers to the karyotype • (46, XX, 46, XY ) 4
Gonadal Sex • The primitive gonad arises from urogenital ridge at approximately 4 to 5 weeks' gestation. 5
Gonadal Sex • The primitive gonad remains bipotential until about 40 days' gestation. 6
Testis Determination One of the first and most significant events in testis determination is SRY. 7
Ovarian Development • Ovarian development is an active process that requires expression of a set of specific genes: ü DAX 1 ü WNT 4 ü RSPO 1 8
Phenotypic Sex • The developing gonad produces several steroid and peptide hormones that mediate sexual differentiation and result in the phenotypic sex seen at birth. 9
Female Sexual Differentiation 10
Phenotypic Sex Female Sexual Differentiation internal genitalia • Müllerian structures persist to form: ü Fallopian tubes ü Uterus ü Upper portion of the vagina. 11
Phenotypic Sex Female Sexual Differentiation internal genitalia The lack of local testosterone production leads to degeneration of wolffian structures. 12
Phenotypic Sex Female Sexual Differentiation external genitalia 13
Disorders of Sex Development 14
Definition • Infants with a congenital discrepancy between external genitalia, gonadal and chromosomal sex are classified as having a disorder of sex development. 15
Disorders of Sex Development • Some DSDs present with abnormalities of the external genitalia (ambiguous genitalia). • Many of these individuals present as newborns with an atypical genital appearance often termed "ambiguous genitalia".
Classification Sex Chromosome DSD 46, XY DSD 46, XX DSD 17
46, XX DSD 18
Etiology of 46 xx DSD q A : Androgen Excess • • • 19 Congenital adrenal hyperplasia Aromatase deficiency Glucocorticoid receptor gene mutation Maternal source ( virilizing tumors e. g. luteoma) Androgenic drugs (progestron , testosterone , …)
Etiology of 46 xx DSD q A : Androgen Excess • • • 31 Congenital adrenal hyperplasia Aromatase deficiency Glucocorticoid receptor gene mutation Maternal source ( virilizing tumors e. g. luteoma) Androgenic drugs (progestron , testosterone , …)
32
Congenital adrenal hyperplasia • • 33 21 -Hydroxylase deficiency ( salt wasting) 11 Hydroxylase deficiency 3 BHSD deficiency ( salt wasting) POR deficiency
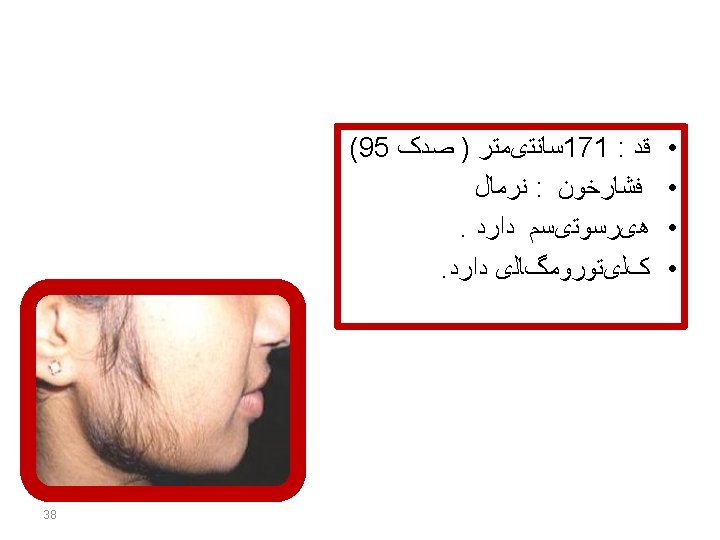
: • آﺰﻣﺎﻳﺸﺎﺕ ﺗکﻤیﻠی Testosterone = high 17 OHP = high DHEAS = NL Cortisol = low 35
: • آﺰﻣﺎیﺸﺎﺕ ﺍﺭﺳﺎﻟی • • 42 Na = NL K = NL Cortisol = NL 17 OHP = NL Testosterone = high Androstenedione = high Estradiol = low
Etiology of 46 xx DSD q A : Androgen Excess • • • 44 Congenital adrenal hyperplasia Aromatase deficiency Glucocorticoid receptor gene mutation Maternal source ( virilizing tumors e. g. luteoma) Androgenic drugs (progestron , testosterone , …)
45
Aromatase deficiency Ø Virilization since birth Ø Further virilization after birth Ø Ovarian failure to synthesize estrogen Ø Maternal serum levels of estrogen : very low Ø Serum levels of androgens : high 46
Aromatase deficiency Ø Large ovarian cysts bilaterally in ultrasonography. Ø Tall stature Ø Delay bone age 47
: • آﺰﻣﺎیﺸﺎﺕ ﺍﺭﺳﺎﻟی • • • 53 Na = NL K = LOW Cortisol = high ACTH = high Testosterone = high
Etiology of 46 xx DSD q A : Androgen Excess • • • 56 Congenital adrenal hyperplasia Aromatase deficiency Glucocorticoid receptor gene mutation Maternal source ( virilizing tumors e. g. luteoma) Androgenic drugs (progestron , testosterone , …)
Glucocorticoid receptor gene mutation Ø Mutation in the GR Ø Elevated cortisol levels Ø High ACTH Ø HTN Ø Hypokalemia Ø Elevated levels of adrenal androgens 57
Etiology of 46 xx DSD q B : Disorders of ovary development • Gonadal dysgenesis ( Turner syndrome & …. ) • Ovotesticular DSD ( True hermaphrodism ) • Testicular DSD ( 46, xx males ) 58
Etiology of 46 xx DSD q C : Other condition • Associated with GU and GI tract defects ( Mayer Rokitansky , …. ) 59