42 Immunodeficiencies I Immunology 297 September 9 2015

#42 Immunodeficiencies I Immunology 297 September 9, 2015 Ikuo Tsunoda, MD, Ph. D. Department of Microbiology and Immunology LSUHSC E-mail: itsunoda@hotmail. com Homepage: http: //tsunodalaboratory. web. fc 2. com/

Concepts Immunodeficiencies occur when one or more components of the immune system is defective Primary immunodeficiency disease (PID): Caused by a genetic mutation that affects any gene that controls the immune responses

Concepts Immunodeficiencies occur when one or more components of the immune system is defective.

Concepts Immunodeficiencies occur when one or more components of the immune system is defective. Secondary immunodeficiency: Acquired as a consequence of other diseases, or are secondary to environmental factors such as starvation, or are an adverse consequence of medical intervention eg. , infectious agents malnutrition hematopoietic tumors transplants

Immunodeficiency research Understand “normal” from “abnormal” or “abnormal” from “normal” • Gain insights into components of the immune system that are important in • Allergy • Abnormal proliferation of lymphocytes • Autoimmunity • Cancer • Infections • Interaction between different cell types contributes to the immune response and to the development of T and B cells • Redundancy of defense mechanisms against infections • A defect compensated by other components • Discovery of defective gene and molecular basis of immune responses, revealing new information about diagnosis, genetic counseling, and gene therapy
 • Around 50, 000 new cases of PID")
Primary immunodeficiency diseases (PIDs or PIDDs) • Around 50, 000 new cases of PID are diagnosed in the US each year • Up to 1 in 2000 live births carry PIDs • At infancy, there is a 5: 1 predominance of males over females • Many of the PIDs are X-linked • With the exception of selective Ig. A deficiency (1: 333 to 1: 700), PIDs are rare • Agammaglobulinemia 1: 50, 000 • SCID 1: 10, 000 to 1: 100, 000 • Abnormalities of more than 120 distinct genes account for more than 150 different forms of PID (Gela et al. , 2007) • The International Union of Immunological Societies (IUIS) Expert Committee for Primary Immunodeficiency updates a classification of PIDs every 2 years

The consequence of the PID depends on the stage of development that is affected
 • Identical clinical conditions are caused by mutations in different immune")
Primary immunodeficiencies (PIDs) • Identical clinical conditions are caused by mutations in different immune system genes • SCID caused by mutations in 12 different genes • Hyper Ig. M syndrome can result from 6 different gene mutations • Phenotypic presentation of mutations in a single gene can be quite different even within the same family • Important to understand that genotype does NOT equate to phenotype • eg. , Di. George syndrome: 85% of patients have exactly the same mutation clinical presentation is very broad – no heart defects normal immune system vs severe congenital heart defects complete absence of T cells
 • Although most PIDs are diagnosed in childhood, ~40% are")
Primary immunodeficiency diseases (PIDs) • Although most PIDs are diagnosed in childhood, ~40% are not diagnosed until adolescence or early adulthood
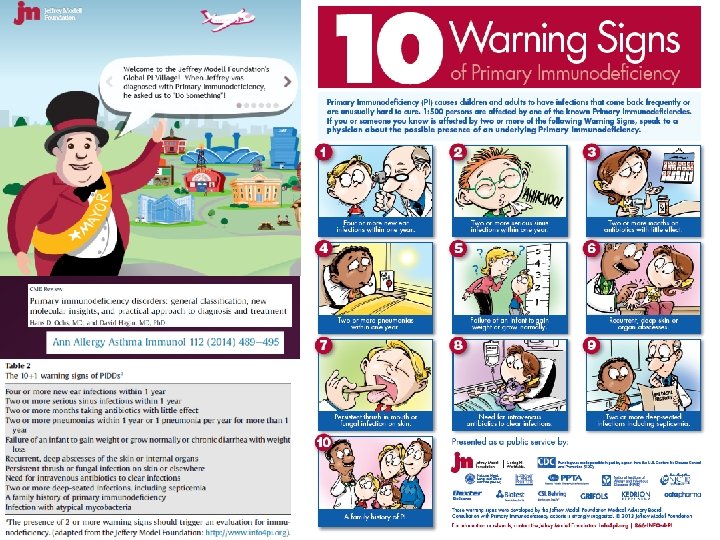

Warning signs for PIDs • 8 or more otitis media infections per year • 2 or more serious sinus infections per year • 2 or more pneumonias per year • recurrent deep infections or infections in unusual areas • infections with opportunistic pathogens • persistent thrush in patients older than 1 year • family history of PID • family history of early childhood deaths Thrush is Candida infection, characterized by white, adherent, painless, discrete or confluent patches in the mouth, tongue, or esophagus

Determining defects in cellular immunity Often present with: • Opportunistic infections [Pneumocystis jirovecii (previously called Pneumocystis carinii), Cryptococcus, Candida spp. ] • Disseminated viral infections (CMV, EBV, VZV) • Failure to thrive, chronic diarrhea, persistent thrush Clinical evaluations: • Complete blood count (CBC) with differential, lymphocyte subsets • Vaccine titers (eg. , tetanus, diphtheria) • Ig levels (Ig. A, Ig. E, Ig. M, Ig. G) • T cell proliferation assays, (eg. , PHA, Con. A, PMA/ionomycin) • Skin testing (eg. , Candida protein)

Determining defects in humoral immunity Often present with: • Recurrent sinopulmonary infections • Encapsulated bacteria (Haemophilus influenza, Pneumococcus spp. , etc. . ) • Parasitic infections (Giardia) • Some virus infections (enteroviruses, papillomavirus) • Chronic diarrhea, poor growth Clinical evaluations: • Vaccine titers (eg. , tetanus, diphtheria) • Ig levels (Ig. A, Ig. E, Ig. M, Ig. G) • B cell subset analysis (eg. , naïve, memory, etc. . )

Determining defects in phagocytosis Often present with: • Recurrent abscesses, abscesses in unusual areas • Recurrent oral ulcers • Severe pneumonias • Catalase+ organisms (eg. , Staph. aureus, Serratia, etc. . ) Clinical evaluations: • CBC with differential • nitroblue tetrazolium (NBT) test for production of oxygen radicals

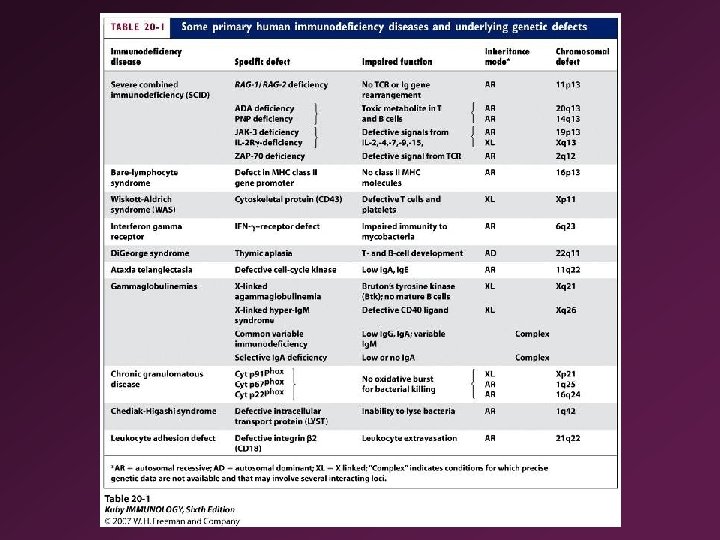
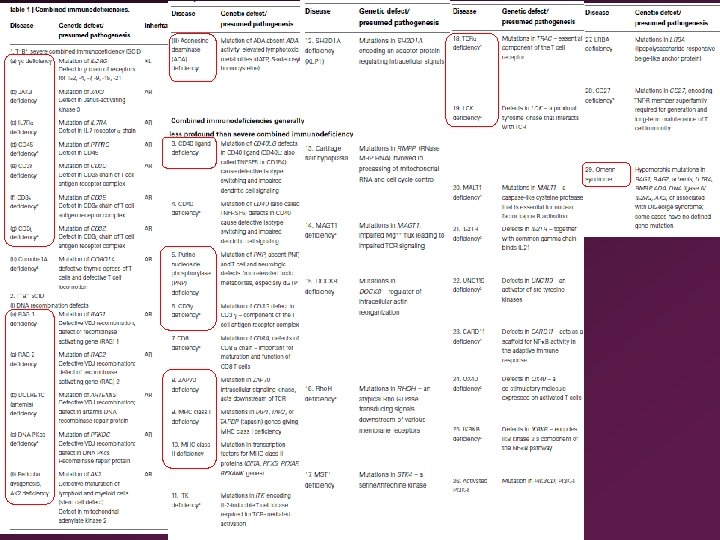
The specific gene defect, the consequence for the immune system, and the resulting disease susceptibilities are listed for some common and some rare human immunodeficiency syndromes. Severe combined immunodeficiency (SCID) can be due to many different defects, as summarized in Figure 13. 8. AID, activation induced cytidine deaminase; ATM, ataxia telangiectasiamutated protein; EBV, Epstein–Barr virus; IKKγ, γ subunit of the kinase IKK; STAT 3, signal transducer and activator of transcription 3; TAP, transporters associated with antigen processing; UNG, uracil-DNA glycosylase; WASP, Wiskott–Aldrich syndrome protein.

April, 2013 report without non-immunological phenotypes Primary Immunodeficiency Expert Committee http: //www. iuisonline. org/iuis/index. php/primary-immunodeficiency-expertcommittee. html

http: //www. omim. org/ a. Fewer than 10 cases
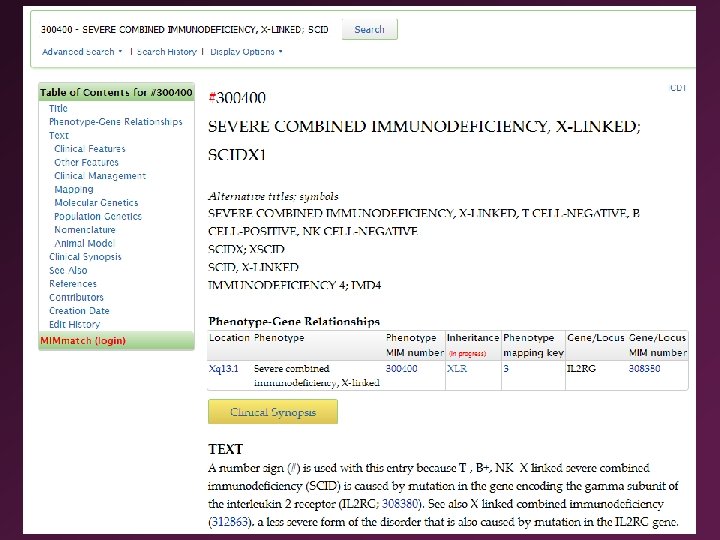

SCIDs: Severe Combined Immunodeficiencies • Typically the most severe types of immunodeficiencies. • Lethal within 6 -12 months if not treated. SCID is often called "bubble boy disease" SCID became widely known during the 1970's and 80's, when the world learned of David Vetter, a boy with X-linked SCID, who lived for 12 years in a plastic, germfree bubble

"The Boy in the Plastic Bubble" Trailer http: //www. youtube. com/watch? v=n. O 5 PC-r. Bs. K 8 The Boy In The Plastic Bubble (1976): http: //www. youtube. com/watch? v=Xs 26 c 4 FDOZY

Seinfeld “The Bubble Boy” Season 4, episode 7
 • Disorders that affects both humoral and cellmediated immunity •")
Severe combined immunodeficiencies (SCID) • Disorders that affects both humoral and cellmediated immunity • Deficiencies of both B and T cells or only T cells • Severe opportunistic infections, death during the first year of life unless given antibody and a bone marrow transplant 1. Lymphocyte precursor cell death due to purine metabolism defect 2. Defective signaling through the common g-chaindependent cytokine receptors 3. Defective V(D)J recombination 4. Defective pre-TCR/TCR signaling

SCIDs: Severe Combined Immunodeficiencies • • Disorders that affect T cells, and sometimes B cells and/or NK cells No effect on myeloid or erythroid cells

Mechanisms of SCID 1. Lymphocyte precursor cell death due to purine metabolism defect (Table 1. 2 iii, 1. 5): ADA (adenosine deaminase) or PNP (purine neucleoside phosphorylase) deficiency results in an accumulation of toxic precursors, which affects developing T and B cells ADENOSINE Purine Catabolism Pathway ADA (adenosine deaminase) INOSINE GUANOSINE HYPOXANTHINE GUANINE PNP (purine nucleoside phosphorylase) Xanthine Oxidase XANTHINE Xanthine Oxidase URIC ACID Guanase PNP (purine nucleoside phosphorylase)

Mechanisms of SCID 1. Lymphocyte precursor cell death due to purine metabolism defect: Adenosine deaminase (ADA) deficiency in 16% of SCID Adenosine metabolites lead to apoptosis of lymphocytes, which causes the immunodeficiency Result : variable, but often results in the absence of T cells, B cells, and NK cells Treatment: Bone marrow transplantation Enzyme replacement therapy polyethylene glycol-modified bovine ADA (PEGADA) weekly administration

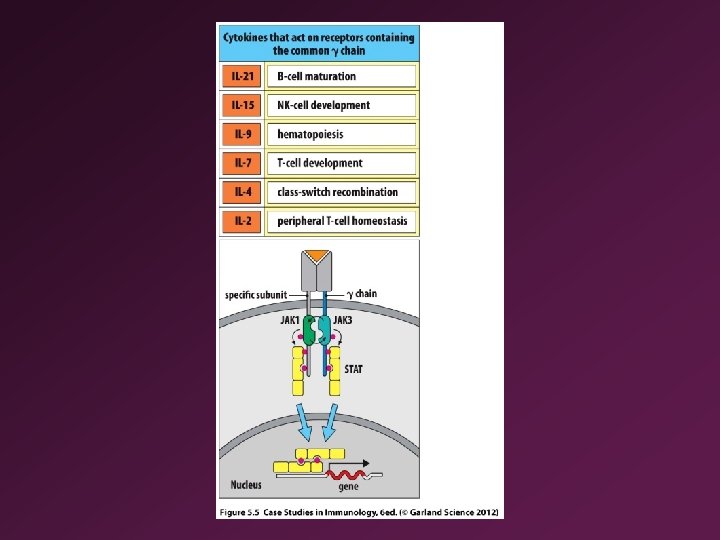
Mechanisms of SCID 2. Defective signaling through the common g-chaindependent cytokine receptors (Table 1. 1 a) : Several cytokine receptors share the common g-chain (gc) subunit: IL-2, IL-4, IL-7, IL-9, IL-15, IL-21

2 -8 Shared subunits in subfamiies of cytokine receptors • Common cytokine-receptor γ chain (γc) chain • Jak 3 associates exclusively with γc chain • γc chain encoded on X chromosome, Jak 3 on autosomal chromosome

Maturation of NK cells requires TAM and IL-15 R • TAM receptors (TYRO 3, Axl, and Mer) expressed on immature NK cells, and their ligands, GAS 6 and protein S are produced by bone-marrow stromal cells • Maturation of NK cells requires TAM and IL-15 R

Mechanisms of SCID 2. Defective signaling through the common g-chaindependent cytokine receptors : Several cytokine receptors share the common g-chain (gc) subunit: IL-2, IL-4, IL-7, IL-9, IL-15, IL-21 Mutations in the common g-chain result in absence of both mature T cells and NK cells. This is the most frequent form of SCID – called SCID-X 1 no T cells or NK cells normal or elevated number of B cells – abnormal immunoglobulin production

Mechanisms of SCID 2. Defective signaling through the common g-chaindependent cytokine receptors Because Janus kinase 3 (JAK 3) mediates signaling from the gc receptors, mutations in JAK 3 result in a SCID phenotype that is indistinguishable from SCID-X 1 gc mutation: X-linked SCID JAK 3 mutation: autosomal recessive SCID IL-7 Rα chain-deficient SCID: T-B+NK+
 shared by IL-2 R and IL-15 R IL-15 Omenn syndrome")
Common beta chain (βc) shared by IL-2 R and IL-15 R IL-15 Omenn syndrome
J recombination (Table 1. 2 i) Mutations in either")
Mechanisms of SCID 3. Defective V(D)J recombination (Table 1. 2 i) Mutations in either RAG-1 or RAG-2 genes impairs the development of T cells and B cells, but not NK cells. T-B-NK+ SCID Mutations in proteins involved in non-homologous end joining repair pathway (eg. , Artemis) prevent resolution of the rearrangement intermediates Radiation-sensitive SCID (RS-SCID)
J rearrangement Gene segments containing recombination signal sequences (RSS) undergo rearrangement beginning with")
RAG-dependent V(D)J rearrangement Gene segments containing recombination signal sequences (RSS) undergo rearrangement beginning with the binding of RAG 1, RAG 2 RAG proteins introduce a DNA doublestranded break, permitting V, D, J gene rearrangement Artemis deficiency results in an inability to repair DNA after double-stranded cuts made by RAG Mice in which either of the RAG genes is knocked out, or which lack DNA-PKcs, Ku, or Artemis, suffer a complete block in lymphocyte development at the generearrangement stage DNA-PKcs: DNA-dependent protein kinase catalytic subunit
 • First described by Gilbert Omenn in")
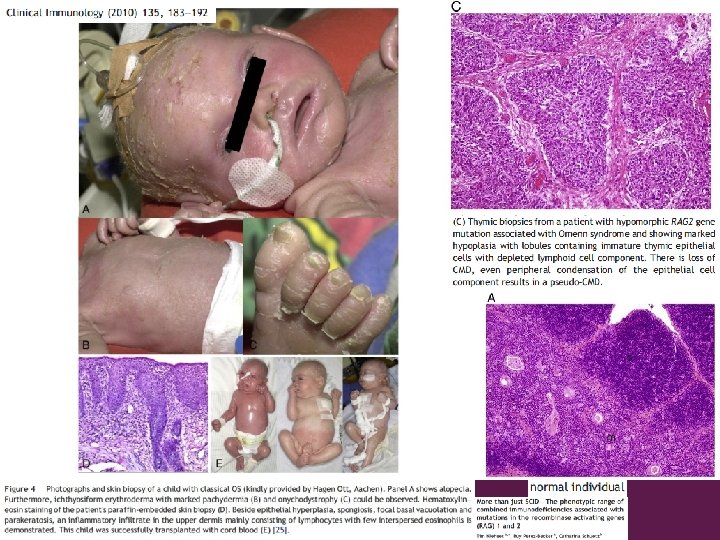
Omenn syndrome: leaky SCID (Table 1. 29) • First described by Gilbert Omenn in 1965 • Chronic diarrhea, pneumonitis [Pneumocystis jirovecii (previously called Pneumocystis carinii), cytomegalovirus, parainfluenza], failure to thrive • Enlarged lymph nodes, hepatosplenomegaly (whereas SCID patients present with paucity or absence of lymph nodes) • Erythroderma, desquamation, alopecia, loss of eyebrows and eyelashes, hypereosinophilia, elevated serum Ig. E • Partial and impaired V(D)J recombinational activity • Hypomorphic mutations in either RAG 1 or RAG 2 • Small amount of RAG protein • Protein loss through the skin and the gut leads to generalized edema and metabolic disturbances • Inflammation in the skin • Fatal unless corrected by bone marrow transplantation

Omenn syndrome: leaky SCID • T cell number is normal • Depressed T cell proliferation to antigens • Depressed humoral immunity • Elevated Ig. E level • NK cells are normal • Abnormal expansion of 1 or more Th 2 type-cell clone, causing inflammation and tissue damage • Abnormal TCR rearrangement results in low-affinity limited repertoire TCRs and therefore skewed Th 2 differentiation (weak TCR stimulation by itself can drive naive CD 4 cells to differentiate into Th 2 cells) • No regulatory T cells, no NKT, no IL-10

 Irradiation-sensitive SCID (IR-SCID) Defects in DNA proteins involved in repairing DNA")
Radiation-sensitive SCID (RS-SCID) Irradiation-sensitive SCID (IR-SCID) Defects in DNA proteins involved in repairing DNA double-strand breaks during antigen receptor rearrangement and by ionizing radiation Very few B and T cells because of a failure of DNA rearrangement Defects in the genes for Artemis, DNA protein-kinase catalytic subunit (DNA-PKcs) IV (Table 1. 2 ib and 1. 2 ic) [and DNA ligase IV (Table 1. 29)] Patients develop cancer
 composed of DNA-PK catalytic subunit (DNA-PKcs) and Ku")
SCID mice DNA-dependent protein kinase (DNA-PK) composed of DNA-PK catalytic subunit (DNA-PKcs) and Ku heterodimer (Ku 70: Ku 80) DNA-PK: Artemis complex has nuclease activity and opens the DNA hairpin Mutation in a DNA protein kinase results in inability of precursor T and B cells to differentiate into mature cells Very commonly used for cellular immunology studies as recipient mice Immune precursors from humans can develop correctly in SCID mice implanted with human thymus tissue …. SCID-hu mice
 •")
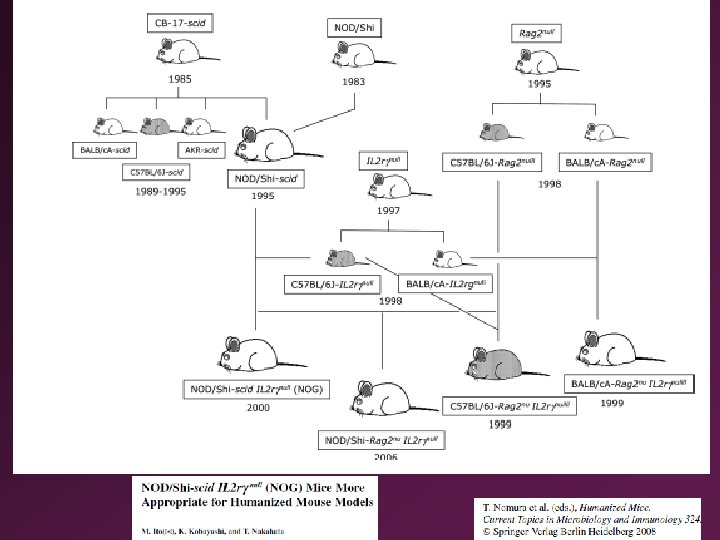
NOG mice: NOD-scid IL 2 rγnull • Discovery of CB-17 -scid (formally Prkcscid) • No functional T or B cells • Mutation of DNA-dependent protein kinase (Prkdc) gene • Normal human hematopoietic cells could be developed (SCIDhu mice), which is difficult with nude mice (no thymus) • NOD-scid • Scid gene introduction into the NOD mice (noneobese diabetes model) • Reduced innate immunity derived from NOD mice: macrophage dysfunction, defect of complement hemolytic activity, reduced NK activity • Humanized mice: human immune system reconstituted from human hematopoietic stem cells in mice • NOD-scid IL 2 rγnull • Elimination of NK cells augment the engraftment of human cells in NOD-scid mice • Lack of NK cells, dendritic cell dysfunction, and other unknown deficiency due to inactivation of IL-2 Rγ gene
")
RAG 2 -/- γc- double mutant mice • Common cytokine receptor γ chain (γc) deficient mice • IL-2, 4, 7, 9, and 15 R • Absence of NK, NKT and γδ T cells • Small number of poorly functioning B cells and αβ T cells • Double mutant mice are completely alymphoid (T-, B-, NK-) • No spontaneous tumor • Normal hematopoietic parameters
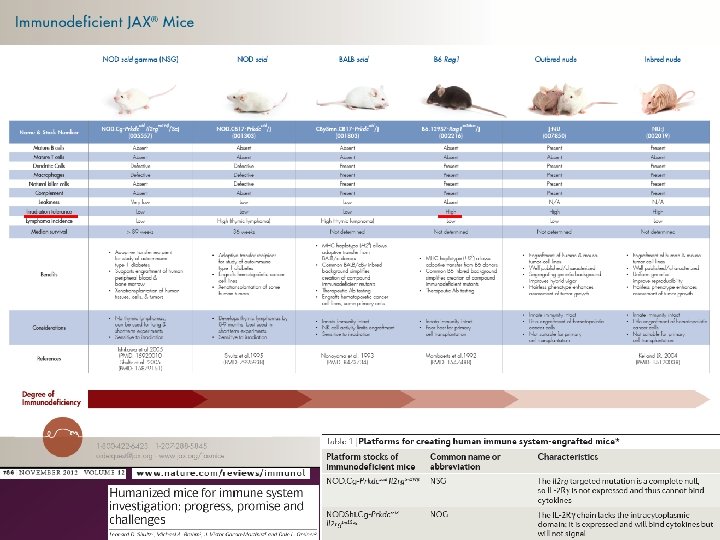

Improvement of immunodeficient mice for humanized mice • Introduction of human growth or differentiation factor • Cross-reactivity of factors between mice and humans may influence human cell engraftment and differentiation • To differentiate and grow myeloid lineage cells: GM-CSF, IL-3, erythropoietin, thrombopoietin • Reconstruction of human secondary lymphoid organs: lymphotoxin, chemokines • Depletion of innate immune cells from immunodeficient mice • Macrophages, dendritic cells, mast cells, neutrophils • Transgenic technique, such as using diphtheria toxin • RNAi technique • Introduction of HLA gene • Lack of cell-to-cell interaction between human T, B cells and macrophages, since T cells are educated in the mouse thymus • HLA transgenic mice

Mechanisms of SCID 4. Defective pre-TCR/TCR signaling: Mutations in critical signaling proteins, such as CD 45, alter T cell development (Table 1. 1 d) (Table 1. 1 e, f, g, 1. 6, 1. 18) (Table 1. 19)

Mechanisms of SCID 4. Defective pre-TCR/TCR signaling : These are rare cases of SCID that are pure T cell deficiencies Failure of T cell development due to defective signaling through the pre-TCR during positive selection. Mutations include: CD 3 d , CD 3 e, CD 3ζ (Table 1. 1 e, f, g) CD 3γ (Table 1. 6) CD 45 (Table 1. 1 d)

Similar defects, but not total SCIDs: Defective pre-TCR/TCR signaling : Mutations in signaling proteins such as ZAP-70 alter T cell development, but some T cells develop normally.

Similar defects, but not total SCIDs: Defective expression of MHC : • MHC class I antigen deficiency (Table 1. 9) • Bare lymphocyte syndrome • No CD 8+ T cells • Mutations in TAP 1, 2 or TAPBP • TAP proteins function to transport peptide antigens from the cytoplasm to Golgi to join MHC class I molecules • MHC class II antigen deficiency (Table 1. 10) • No CD 4+ T cells • CD 8 deficiency (Table 1. 7)
 (Table 2. iii)")
Percentages of SCID in the population (Table 1. 13) (Table 2. iii)
 • Fist described in 1959 • Less")
Reticular dysgenesis (Aleukocytosis, Table 1. 2 ii) • Fist described in 1959 • Less than 2% of SCID • The most severe SCID • Total lack of lymphocytes and granulocytes in blood and bone marrow • Lack of innate and adaptive humoral and cellular immunity • Fatal sepsis within days after birth • Myeloid differentiation is blocked at the promyelocytic stage • Erythro- and megakaryocytic maturation is normal • Mutation in adenylate kinase 2 (AK 2), mitochondrial energy metabolism enzyme • First example of PIDs that is causally linked to energy metabolism (mitochondoriopathy)

The consequence of the PID depends on the stage of development that is affected.

14 -1 Treatment of SCID • Successful gene therapy • Hematopoietic stem cells from patients’ bone marrow are infected with a retrovirus encoding the γc gene • High incidence of leukemia due to integration of the vector sequences next to an oncogene

Severe combined immunodeficiency syndromes
- Slides: 56