4 th lecture Respiratory medicine 2018 Chronic obstructive

4 th lecture Respiratory medicine 2018
 • • • Objective Defind COPD Aetiology of COPD")
Chronic obstructive pulmonary disease (COPD) • • • Objective Defind COPD Aetiology of COPD Pathology Clinical features and diagnosis Treatment and prognosis

• To know the epidemiology , etiology, pathogenesis , clinical presentation, investigation , diagnosis , treatment , complication , prognosis

Definition • A preventable and treatable lung disease with some significant extrapulmonary effects that may contribute to the severity in individual patients.

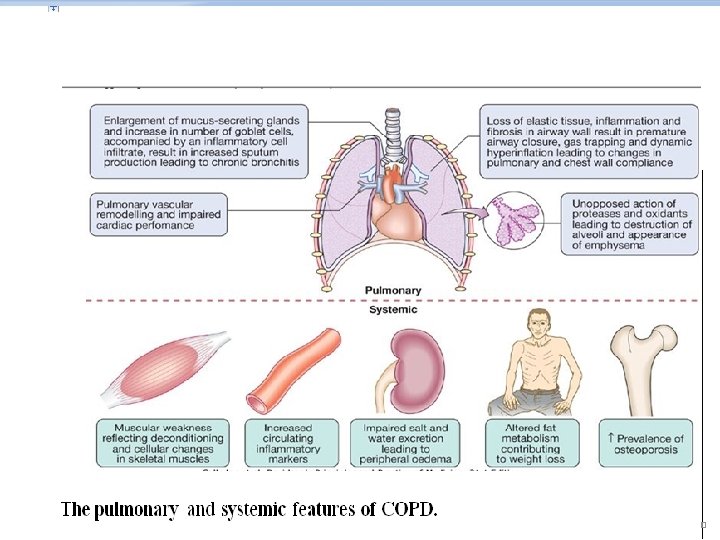
The pulmonary component of COPD Is characterised by • airflow limitation that is not fully reversible. • usually progressive and associated with an abnormal inflammatory response of the lung to noxious particles or gases.

Extrapulmonary manifestations Include • impaired nutrition. • weight loss. • skeletal muscle dysfunction.

Related diagnoses include • Chronic bronchitis • (cough and sputum on most days for at least 3 consecutive months for at least 2 successive years)

Emphysema (abnormal permanent enlargement of the • airspaces distal to the terminal bronchioles, accompanied by destruction of their walls and without obvious fibrosis).

Small airways disease • Airway less than 2 mm.

Epidemiology • • 80 million people world-wide suffer from moderate to severe disease. • In 2005 more than 3 million deaths (5% of deaths globally). • 2020 represent the third most important cause of death world-wide. • increasing tobacco consumption.

Aetiology • Cigarette smoking • It is unusual in those less than 10 pack years (1 pack year = 20 cigarettes/day/year) • individual susceptibility factors are important.

Risk factors for development of COPD Exposures • Tobacco smoke: accounts for 95% of cases in UK • Biomass solid fuel fires: wood, animal dung, crop residues and coal lead to high levels of indoor air pollution • Occupation. • air pollution • Low birth weight. • childhood infections or maternal smoking • Infections. • Low socioeconomic status • Cannabis smoking

Host factors • Genetic factors: α 1 -antiproteinase deficiency. • Airway hyper-reactivity q Note It is unusual to develop COPD with less than 10 pack years (1 pack year = 20 cigarettes/day/year)about 20% of smoker devlope this condition,

Pathophysiology

1 -The changes in compliance mean that collapse of intrathoracic airways during expiration is exacerbated, during exercise as the time available for expiration shortens, resulting in dynamic hyperinflation.

2 -Increased V/Q mismatch • increases the dead space volume and wasted ventilation.

3 -Flattening of the diaphragmatic muscles and an increasingly horizontal alignment of the intercostal muscles.

4 -The work of breathing is therefore markedly increased, first on exercise but, as the disease advances, at rest too.

Pathophysiology of Emphysema May be classified by the pattern of the enlarged airspaces: • centriacinar, • panacinar • periacinar. q Bullae form in some individuals , this results in impaired gas exchange and respiratory failure.
. B. Paraseptal (distal acinar). C. Panacinar (panlobular).")
Anatomic varieties of emphysema. A. Centriacinar (centrilobular). B. Paraseptal (distal acinar). C. Panacinar (panlobular). D. Irregular (scar). The dashed lines mark the edge of the acinus.
 NORMA(")
Pathology of emphysema (A) NORMA(

Who has COPD
 and ‘pink puffer’ (bottom).")
Blue bloater’ (top) and ‘pink puffer’ (bottom).

Clinical features • COPD should be suspected in any patient over the age of 40 years who presents with symptoms of chronic bronchitis and/or breathlessness

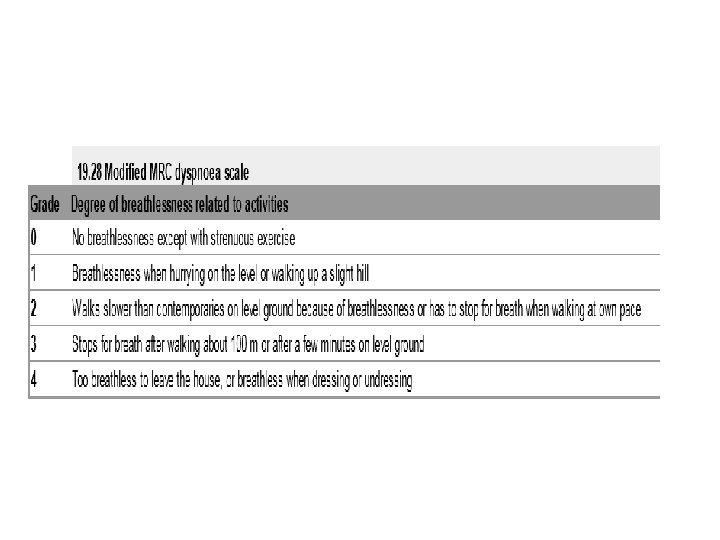
SYMPTOMS • Cough and associated sputum production are usually the first symptoms, often referred to as a 'smoker's cough'. • Haemoptysis. • Breathlessness : the modified Medical Research Council (MRC) dyspnoea scale. • morning headaches, which may suggest hypercapnia.

Physical signs • • • non-specific, Breath sounds are typically quiet; crackles. pitting oedema The body mass index (BMI) is of prognostic significance

Tobacco 'tar'-stained fingers

Hyperinflation

Two classical phenotypes have been described • 'pink puffers' are typically thin and breathless, and maintain a normal Pa. CO 2 until the late stage of disease. • The 'blue bloaters' develop (or tolerate) hypercapnia earlier and may develop oedema and secondary polycythaemia. In practice, these phenotypes often overlap. •

• • • Differential diagnoses chronic asthma. tuberculosis. bronchiectasis. congestive cardiac failure.

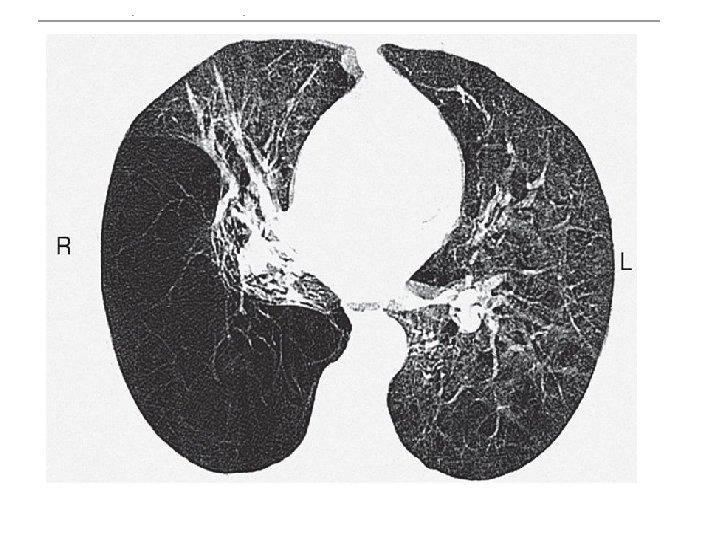
This 42 -year-old man had smoked 20 cigarettes a day since the age of 14. He presented with a 5 -year history of progressive breathlessness and could walk only 100 m. He had severe airway obstruction, with an FEV 1 of 0. 5 l and a transfer factor for carbon monoxide and transfer coefficient reduced to 30% of predicted values. High-resolution CT shows extensive emphysematous bullae with dilated distal airspaces, cysts and destruction of alveolar architecture. Levels of �� 1 -antitrypsin were unrecordable.

Investigations 1 -a chest X-ray is essential to identify alternative diagnoses such as • cardiac failure, • lung cancer. 2 -A full blood count is useful to exclude • anaemia. • polycythaemia. 3 - α 1 -antiproteinase younger patients with predominantly basal emphysema, . •

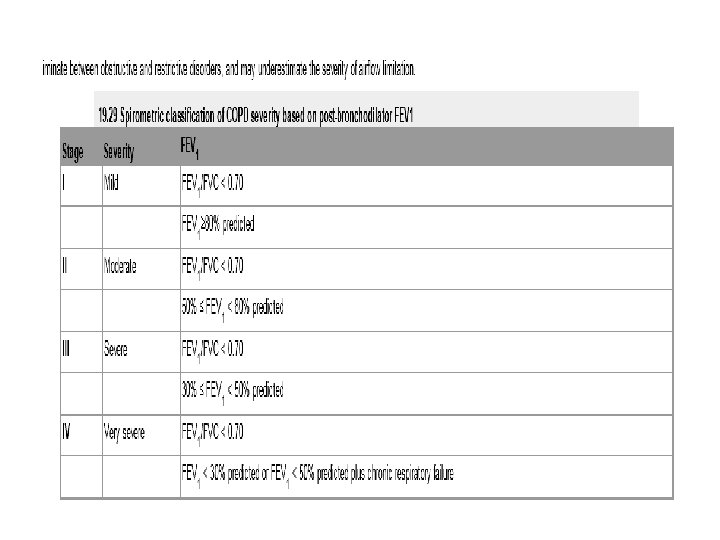
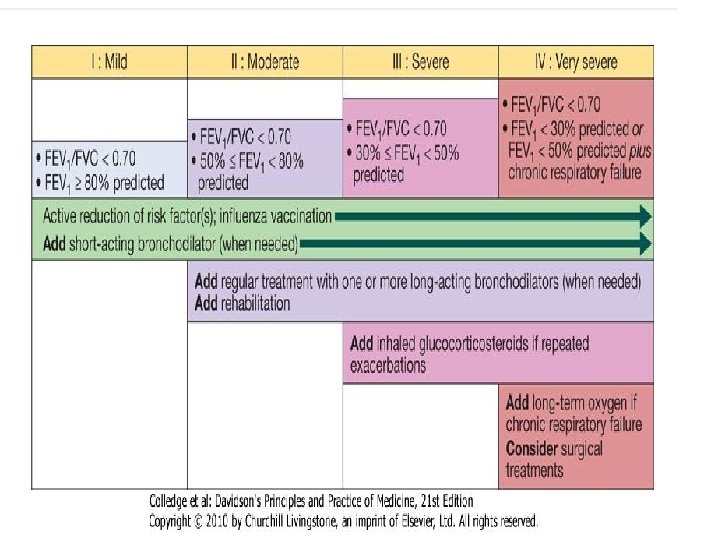
4 -Spirometry the post-bronchodilator FEV 1 is less than 80% of the predicted value and accompanied by FEV 1/FVC < 70%. 5 - peak flow is consistent with COPD. 6 -Measurement of lung volumes by body plethysmography. 7 -The low gas transfer factor suggeste presence of emphysema. 5 - Exercise tests. 6 - Pulse oximetry

Gross emphysema. HRCT showing emphysema most evident in the right lower lobe.

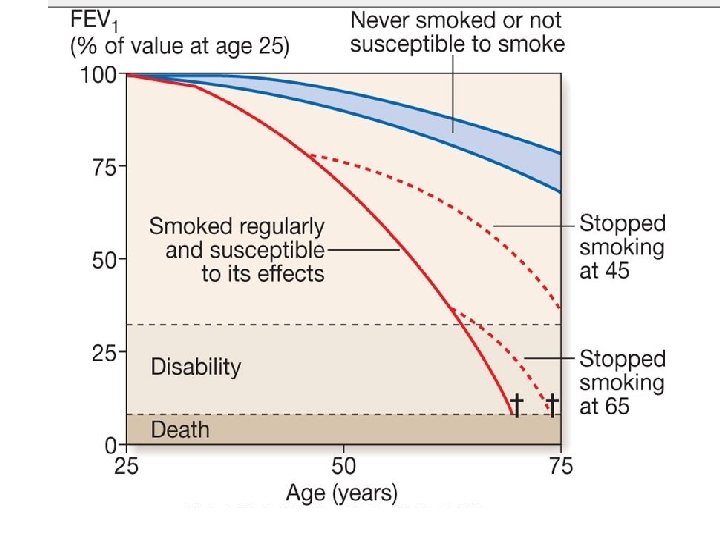
Management I---Smoking cessation and COPD • 'Sustained smoking cessation in mild to moderate COPD is accompanied by a reduced decline in FEV 1 compared to persistent smokers. '

II-Bronchodilator • central to the management of breathlessness. v The inhaler q Mild disease. Ø Short-acting bronchodilators. • β 2 -agonists salbutamol and terbutaline. • the anticholinergic ipratropium bromide.

q moderate to severe disease. Ø Longer-acting bronchodilators, • the β 2 -agonists salmeterol and formoterol. • the anticholinergic tiotropium bromide.

Oral bronchodilator. • Theophylline preparations improve breathlessness and quality of life, • Bambuterol , a pro-drug of terbutaline, is used on occasion. • phosphodiesterase inhibitors
. • Oral corticosteroids are useful during exacerbations.")
Corticosteroids • Inhaled corticosteroids (ICS). • Oral corticosteroids are useful during exacerbations.

• Pulmonary rehabilitation
")
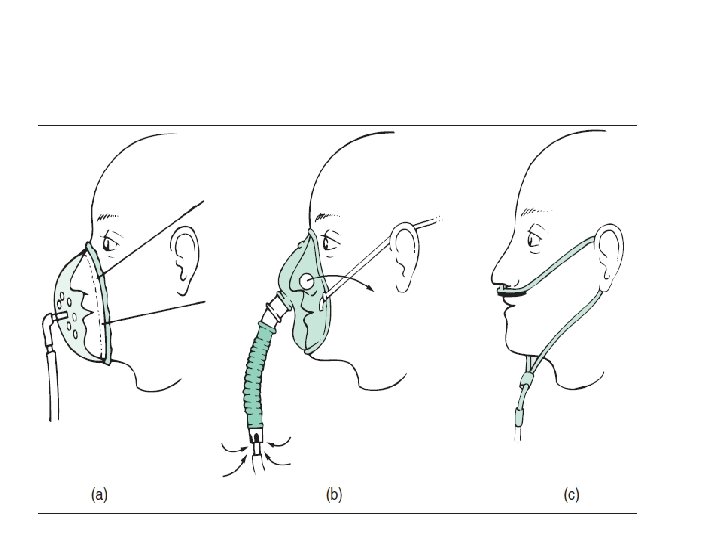
Oxygen therapy Long-term domiciliary oxygen therapy (LTOT)

• Arterial blood gases measured in clinically stable patients on optimal medical therapy on at least two occasions 3 weeks apart: • Pa. O 2 < 7. 3 k. Pa (55 mm. Hg) irrespective of Pa. CO 2 and FEV 1 < 1. 5 L • Pa. O 2 7. 3 -8 k. Pa (55 -60 mm. Hg) plus pulmonary hypertension, peripheral oedema or nocturnal hypoxaemia • patient stopped smoking. • Use at least 15 hours/day at 2 -4 L/min to achieve a Pa. O 2 > 8 k. Pa (60 mm. Hg) without unacceptable rise in Pa. CO 2.
. • Lung")
• Surgical intervention • bullectomy. • lung volume reduction surgery (LVRS). • Lung transplantation.

Other measures • an annual influenza vaccination • pneumococcal vaccination. Treat o Obesity. o poor nutrition. o depression. • Mucolytic therapy such as acetylcysteine, • antioxidant agents.

• Palliative care • Morphine preparations • benzodiazepines in low dose may reduce anxiety.

Prognosis q. COPD usually progressive. • inversely related to age • directly related to the post-bronchodilator FEV 1. q poor prognostic indicators • weight loss • pulmonary hypertension. •
 the include following variables • • the body mass index (B),")
A (BODE index) the include following variables • • the body mass index (B), the degree of airflow obstruction FEV 1 (O), a measurement of MRC dyspnoea scale (D) Distance walked in 6 min (m)exercise capacity (E).

Causes of death • Respiratory failure. • cardiac disease. • lung cancer.

Acute exacerbations of COPD • • • characterised by an increase in symptoms. deterioration in lung function and health status. are usually triggered by bacteria, viruses or a change in air quality. respiratory failure and/or fluid retention and represent an important cause of death. Indication of refferal to hospital • The presence of cyanosis, • peripheral oedema • an alteration in consciousness should prompt referral to hospital.

Oxygen therapy • • In patients with an exacerbation of severe COPD, high concentrations of oxygen may cause respiratory depression and worsening acidosis. • Controlled oxygen at 24% or 28% should be used with the aim of maintaining a Pa. O 2 > 8 k. Pa (60 mm. Hg) (or an Sa. O 2 > 90%) without worsening acidosis.

1 -Bronchodilators • Nebulised short-acting β 2 -agonists combined with an anticholinergic agent (e. g. salbutamol with ipratropium). • usually safe to drive nebulisers with oxygen, but if concern nebulisers may be driven by compressed air and supplemental oxygen delivered by nasal cannula.

2 -Corticosteroids • Oral prednisolone reduces symptoms and improves lung function. • Currently, doses of 30 mg for 10 days are recommended but shorter courses. • Prophylaxis against osteoporosis.

3 -Antibiotic therapy • • little evidence for the routine administration of antibiotics. • They recommended for patients reporting an increase in sputum purulence. • breathlessness. Choice • an aminopenicillin • a macrolide. • Co-amoxiclav.

4 -Non-invasive ventilation • If, despite the above measures, the patient remains tachypnoeic and acidotic (H+ ≥ 45/p. H < 7. 35), then NIV should be commenced. • Mechanical ventilation.

5 -Additional therapy • peripheral oedema; responds to diuretics. • the respiratory stimulant doxapram. • Discharge • clinically stable.

THANK YOU

Q QUIZE •
- Slides: 67