4 Seasons Lecture Bon Apptit Part 1 Pediatric

4 Seasons Lecture Bon Appétit !

Part 1 Pediatric Pleural Diseases By Prof Malak Shaheen (MD, MSc Pediatrics, Ph. D Pediatrics) (MSc Critical Care Medicine)

Objectives of this lecture: Recognize normal pleural anatomy & physiology in children. Identify different pleural diseases in children Manage pleural diseases in children
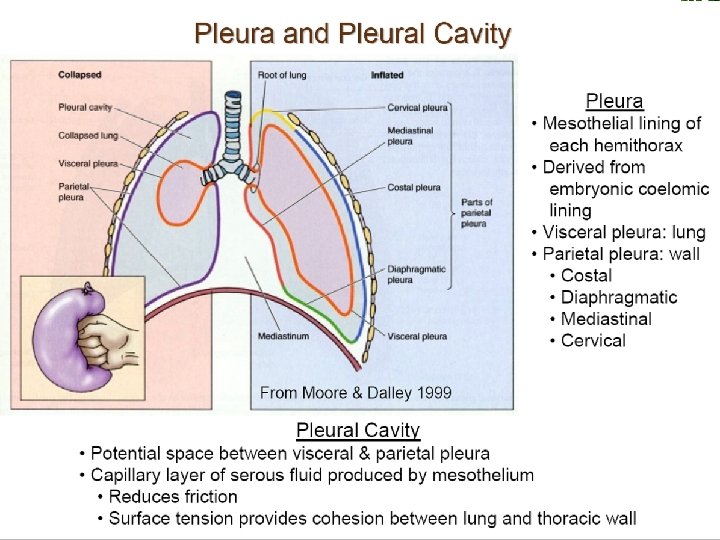

Pleural Physiology: Fluid circulation Pleural fluid 0. 3 ml/kg In continuous circulation Negative pressure Normal Pleural Fluid; ph 7. 6, prot <2 gm, few cells, LDH <50%

Function of pleural space The pleural space couples the lung with the chest wall and provides an integrated respiratory system.
 Low oncotic pr;")
Causes of Pleural Effusion Transudate High systemic venour pr; (eg. HF) Low oncotic pr; (hypoprot. ? ? ? ) Exudate Increased capillary permeability; (capillary wall insult) eg; pulm infections, pleural infections, adjecent inflammation, CT diseases, malignancy. Iatrogenic; trauma Chylothorax

What is empyema? = presence of pus in pleural cavity Occurs with severe infections Infection initiates massive inflammotory cellular influx, activation of coagulation cascade, reduction of fibrinolysis & massive fibrin deposition in pleural space. Very thick pleural collection blocks lymphatic pores and prevent pleural drainage.

Symptoms & Signs General: . . . Local: Breathlessness Pain General: cause Local: Inspection (Litten sign) Palpation (Trachea) Percussion (Tone) Auscultation (sounds, rub, adv sounds)

Investigations
 Cytology Microbiological (G stain & culture) Other; TG,")
Thoracocentesis fluid analysis Chemistry (protein, LDH) Cytology Microbiological (G stain & culture) Other; TG, ADA, …
 or moderate")
TTT Cause Intercostal tube application; indicated if – empeyma (of any amount) or moderate to severe pleural effusion (what is the care of the tube? ) Fibrinolysis Video assisted thorascopic Surgery (VATS) Open surgery; decortication operation

Antibiotics All cases should be treated with intravenous antibiotics and must include cover for S pneumoniae. Broader spectrum cover is required for hospital-acquired infections, as well as those secondary to surgery, trauma and aspiration.

Pneumothorax Accumulation of extrapulmonary air within the chest May be primary or secondary May be sponteneous, traumatic, or iatrogenic Onset is usually abrupt and severity of symptoms depends on the extent of collapse lung

Pneumothorax

Symptoms & Signs General: . . . Local: Breathlessness Pain General: cause Local: Inspection (Litten sign) Palpation (Trachea) Percussion (Tone) Auscultation (sounds)
 Pleurodesis Treatment of the")
Pneumothorax Observation 100% oxygenation Simple aspiration Thoracostomy (Intercostal tube Drain) Pleurodesis Treatment of the cause; if 2 ry

Specific situation “Tension Pneumothorax” Occurs when air accumulates in the pleural space through a leak with a one way vavle Air enters with each inspiration and the intra pleural pr increases Pr compresses the lungs and mediastinum great vs ac HF TTT = High flow O 2 + wide gauge canula application in 2 nd ICS - MCL

Part 2 Bronchiectasis in children

Objectives of the lecture; Define bronchiectasis Diagnose bronchiectasis Manage bronchiectasis in children

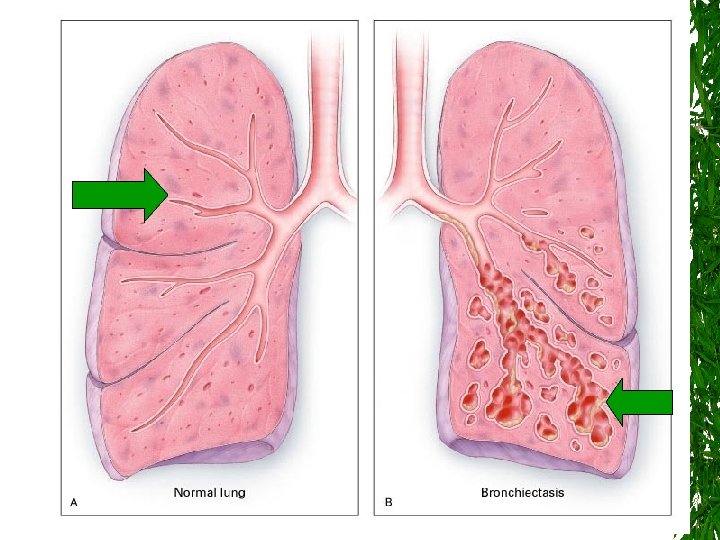
What is the meaning of Bronchiecatsis?

Bronchi= Bronchial Tree ectasis = Dilation “Chronic dilation of the bronchi marked by expectoration of mucopurulent matter. ” Dorland’s Illustrated Medical Dictionary 28 th Ed. , W. B. Saunders Company
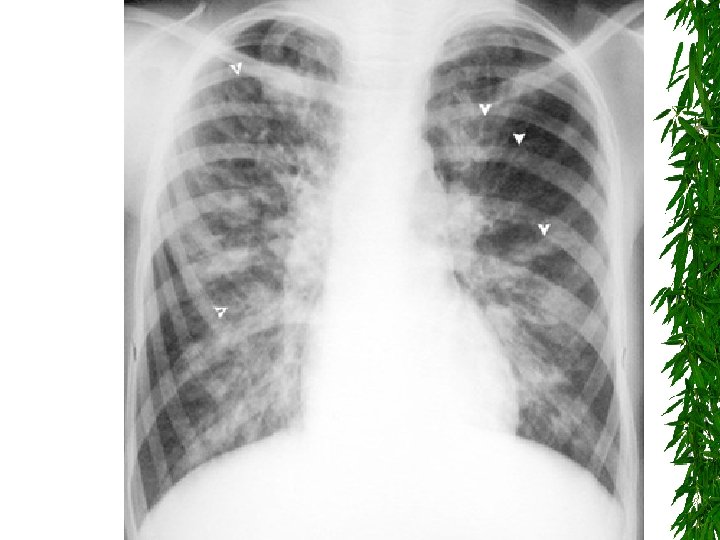
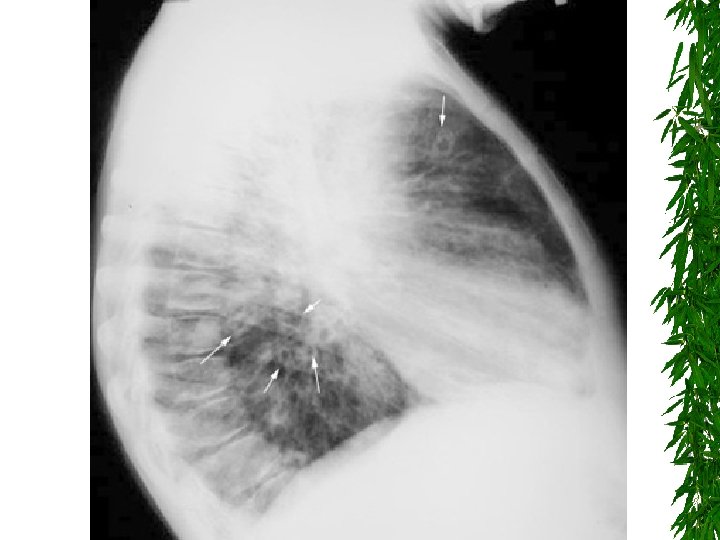
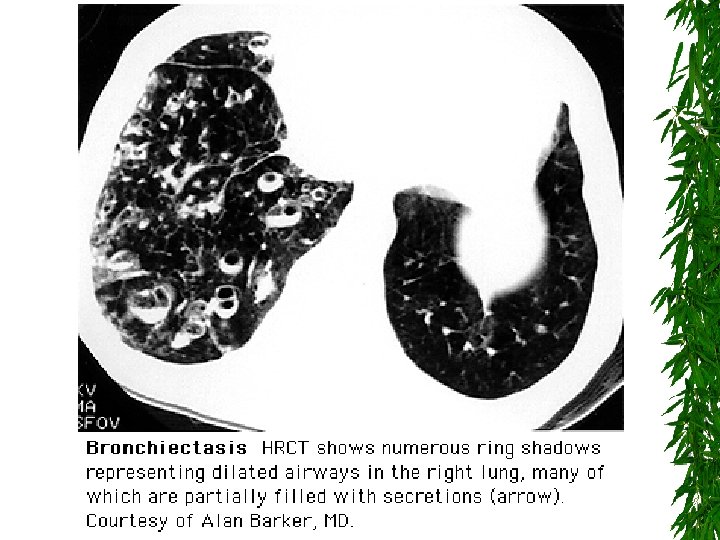

Characteristic central bronchiectasis 2/2 ABPA

Note characteristic location in the upper lobes and superior segments of lower lobes

Pathogenesis Always starts with chronic infection of bronchi Cause of this chronic infection is one or more of the following; Resistent Organism infection Stasis of bronchial secretions (physical/functional) Immunocompromisation (host defence defect; congenital; acquired or iatrogenic)

Bronchiectasis Worldwide, LRTI infection is the primary cause M. Tuberculosis B. Pertussis ABPA Strep. Pneumoniae Staff. Aureus

Immunodeficiency Congenital; AB defects. SCID Acquired; HIV Following chemotherapy Ataxia telangectasia

Stasis of Bronchial secretions Obstruction of bronchi: Foreing body aspiration Tumor LN Congenital airway/lung defect Fibrosis Functional stasis; PCD CF Chronic aspiration

This chronic infection will result in chronic inflammation of the bronchi

Inflammation Characteristics across etiologies: - Persistent - Neutrophil dominant - Pro-inflammatory cytokines (IL 8, IL-1, TNF-a) - Low anti-inflammatory cytokines (IL-10)

Sequence of Persisten Chronic Airway Inflammation Altered Airway Milieu Proteolytic damage -e. g. cleaved receptors -impaired macrophage function Oxidant stress -low antioxidants associated with worse disease -dysregulation of signaling and cellular function

Fibrosis + dilation + Airway damage = Bronchiectasis Cylindrical or tubular bronchiectasis Varicose saccular or cystic bronchiectasis

HIV/AIDS Childhood Infections Chemo-Immunosuppression M. Tb. Innate Deficiency Infection Auto-Immune ABPA Inflammation Bronchiectasis Altered development Impaired Clearance

When to suspect bronchiectasis? Chronic cough, sputum Coarse rales Persistent respiratory symptoms Recurrent pneumonia Progressive obstructive lung disease Funny bugs (? )

Clinical Characteristics Focal Sputum production – Mild <15 cc/d – Moderate 15 -150 cc/d – Severe >150 cc/d Hemoptysis Dyspnea Chest pain Systemic Malnutriton/wasting Chronic Inflammation – – “gammaglobulinemia” CRP ESR anemia
 Bronchoscopy Microbiology Pulmonary function")
Investigations Diagnosis of bronchiectasis and its severity; Imaging (CXR, HRCT) Bronchoscopy Microbiology Pulmonary function Diagnosis of the cause; Sweet chloride test p. H metry Immune system test Ciliary brush test HIV test Bronchogram now is OBSOLETE…………

Vicious loops Infection Bronchial Obstruction Inflammation Bronchiectasis

Vicious loop Antibiotics tobramycin Infection Bronchial Obstruction Inflammation Clearance Anti-inflammatory Albuterol, DNase, Therapy vest Inhaled steroids Bronchiectasis

Bronchiectasis Therapy Decrease inflammation 1. Antibiotics 2. Clearance Flutter, IPPV, Vest, Bronchodilators, hypertonic saline 3. Anti-inflammatory chemotherapy 1. 4. Steroids, macrolides, interferon-gamma, ibuprofen Surgical resection

Bronchiectasis Therapy 1 - Antibiotics Episodic or suppressive antibiotics? Both.

Bronchiectasis Therapy Antibiotics Pro Decrease inflammation Slow progression Eradication? Con Select resistance Cost Side effects adherence difficult (e. g. Huong et al. )

Bronchiectasis Therapy 2 - Decrease inflammation Clearance Immunomodulatory chemotherapy proposed therapies: Steroids Macrolides, tetracyclines interferon-gamma ibuprofen

3 - Bronchopulmonary Hygiene Removal of respiratory secretions is beneficial Chest percussion and postural drainage Chest clapping or cupping Inflatable vests or mechanical vibrators Oral devices that apply positive endexpiratory pressure maintain the patency of the airway during exhalation

Maintaining adequate systemic hydration, enhanced by nebulization with saline, Acetylcysteine delivered by nebulizer thins secretions aerosolized recombinant human DNase (rh. DNase) in patients with cystic fibrosis

CPT

")
Vest Therapy (High Frequency Chest Wall Oscillation)

Flutter

Acapella

IPV- Intra-pulmonary percussion ventilation

Nebulizers

Alternative forms of airway clearance techniques

Bubble PEP

4 - Surgery Localised bronchiectasis Proximal obstructive lesion Massive hemoptysis Recurrent infections

Summary Diagnosis History Prior infections, exposures Time course Other manifestations? Chest Imaging Define region, pattern Sputum culture Determine causal disease sweat testing immune testing serologic testing Management Treat bronchiectasis Clearance Antibiotics Immune-modulation Balance burden of disease vs burden of therapy (Sputum, Symptoms, PFT’s, Weight, Xrays) Other… Underlying disease therapy Transplantation Management of complications Collapse, plugs, hemoptysis

Part 3 Childhood Pulmonary Functions Tests By Dr Malak Shaheen childshaheen@yahoo. com
. John Hutchinson (1811 -1860). The 20 th Century (1850 -1950). Children")
Earliest trial (1681). John Hutchinson (1811 -1860). The 20 th Century (1850 -1950). Children testing (1960 s). Infants and preschool children testing (1980 s).

How to perform PFT in children? Place Child Equipments Operator Reference Values & interpretations (QC)
 Bronchial")
Which Technique? Pediatric PFT Lung Volumes and Ventilation Passive Respiratory Mechanics (Rres &Cres) Bronchial Responsiveness Active Tell me first; What is your clinical Q ? Others
 study (VT, control of")
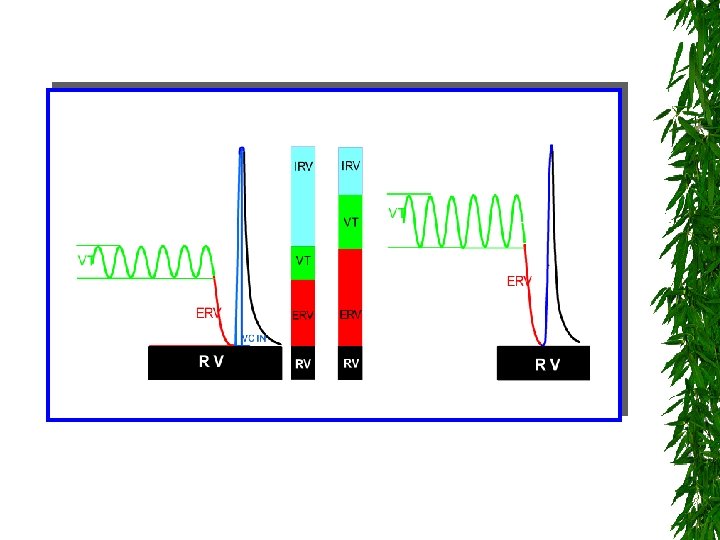
First: Lung volumes and Ventilation Studies 1. Tidal Breathing (TB) study (VT, control of breathing, Tidal flow volume loops) 2. Multiple breath washout (MBWSF 6) test FRC Gas mixing efficiency (LCI)
 - TLC (special circumstances) Master.")
3. Body plethysmography for: - FRC (with tidal breathing) - TLC (special circumstances) Master. Screen body
 A: Passive (Tidal breathing): 1. Plethysmography (Raw &")
Second: Respiratory Mechanics (Rres & Cres) A: Passive (Tidal breathing): 1. Plethysmography (Raw & s. Raw) 2. Occlusion Tech (Rres) 3. Interruption Tech (Rint) 4. Forced oscillation Tech (FOT) (Zres) e. g. IOS
: 1. Spirometry (Special considerations with young children)")
B: Active (Forced Expiratory Tech. ): 1. Spirometry (Special considerations with young children)

How to interpret in children? FEV 1 % Normal Restrictive 80% Mixed Obstructive 80% %FVC Problem: FEV 1 may not be always recorded!
 techniques = squeeze technique -")
2. Partial forced expiratory maneuver Rapid Thoracic Compression (RTC) techniques = squeeze technique - RTC with Tidal breathing (TBRTC) - RTC with external raised volume (RVRTC)
 Which PFT technique? Infant: Tidal RTC")
Third: Bronchial responsiveness (BD, BC and Exercise test) Which PFT technique? Infant: Tidal RTC Preschool child: Rint, FOT, s. Raw School children: Spirometry, Plethysmograph Provocation test? Chemical: both direct (H or M) and indirect (A or H) Physical: cold or dry air Exercise (? )
 using CO (DLco, VA,")
Fourth: Other tests CO Diffusion Test ; Diffusion capacity (DL) using CO (DLco, VA, TLco, Kco) Sa. O 2 ABG Fe. NO PEFM Indirect calorimeter (Canopi test)

PEFM Best PEF X 0. 8 = Lower limit of green Best PEF X 0. 5 = Lower limit of yellow Diurnal Variability: To differentiate between mild intermittent (<20%) and mild persistent (20 -30%) asthma

Thank You Drmalak_shaheen@med. asu. edu. eg
- Slides: 75