4 Seasons Lecture Bon Apptit Part 1 Childhood

4 Seasons Lecture Bon Appétit !
 Dr. Malak Shaheen (Ph. D Pediatrics,")
Part 1 Childhood Interstitial lung Disease (ch. ILD) Dr. Malak Shaheen (Ph. D Pediatrics, MSc Critical Medicine)

What is ch. ILD Syndrom? “Pneumonitis” Alveoli & perialveolar tissues Impaired gas exchange

What are common features of ch. ILD? Persistent 3 of the following 4 ≥ 1 month: 1 - Respiratory symptoms 2 - Impaired gas exchange 3 - Diffuse/Patchy radiological chest abnormality 4 - Adventitious sounds

Fan Staging of ch. ILD Asymptomatic Symptomatic with normal Sa. O 2 Symptomatic with nocturnal or exercise-induced ↓Sa. O 2 4. ↓Sa. O 2 at rest 5. Pulmonary hypertension 1. 2. 3.
 Infectious Metabolic disorders Aspiration (GORD) Surfactant")
Causes of ch. ILD Lymphoproliferative disorders (including HIV) Infectious Metabolic disorders Aspiration (GORD) Surfactant disorders Environmental (hypersensitivity Neurocutaneous pneumonitis) syndromes Drug-induced Idiopathic pulm Neoplastic diseases (&LCH) hemosidrosis

Causes of ch. ILD Collagen vascular disease Pulmonary vasculitis syndromes Radiation-induced Amyloidosis Graft-versus-host disease cont…. ARDS (recovering phase) Hypereosinophilic syndromes Pulmonary venoocclusive disease Sarcoidosis With chronic liver, kidney, bowel diseases
 disease Primary ciliary dyskinesia")
DD to rule out include: Cystic fibrosis Asthma Cardiac (heart) disease Primary ciliary dyskinesia Scoliosis and chest wall abnormalities Neuro-muscular disease/Neurocut dis Immune deficiency TB Developmental abnormalities (BPD - Alveolar capillary dysplasia- Pulm hypoplasia)

Does ch. ILD differ from ad. ILD? 1. 2. 3. 4. 5. Immune system responces, cytokines and growth factors Histologic classification Specific types Rarer and less stereotyped More difficult to manage Children Adult

Is there one test to diagnose ch. ILD? 1. 2. 3. 4. First round investigations: Imaging Lung functions Sa. O 2 Blood tests (CBC, ESR, Immune, Serology, PCR, RAST, ACE, HIV) 5. 6. 7. 8. 9. 10. C&S /PCR Sweat chloride test. p. H study/Contrast swallow ECG and ECHO Ciliary Brush Biopsy Urine for CMV PCR

Is there one test to diagnose ch. ILD? Second round investigations: 1. 2. 3. 4. 5. 6. Bronchoscopy and BAL for cytology (LCH, iron laden macrophages, PAP) and cultures Prone Oesophagram for H type fistula Videofluroscopy for aspiration evidence Cardiac Cath Detailed lymphocyte function tests TB –Elispot test

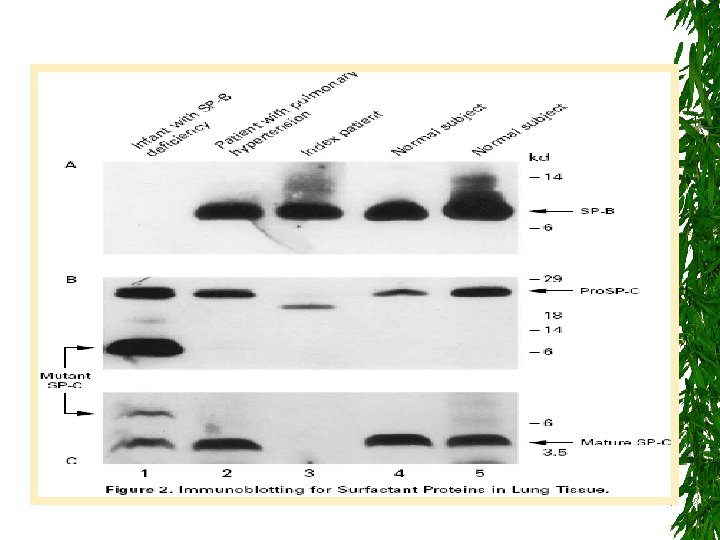
Is there one test to diagnose ch. ILD? Third round investigations: 1. Lung biopsy (Transbronchial, percutaneous, thoracoscopic, open lung) CT guided from affected patch and unaffected patch. Special stains (eg. Bompesin or PAS) Immunoblotting for sufactant proteins at lung biopsy Electron microscopy study of biopsy 2. DNA for mutations in SPB, SPC and ABCA 3

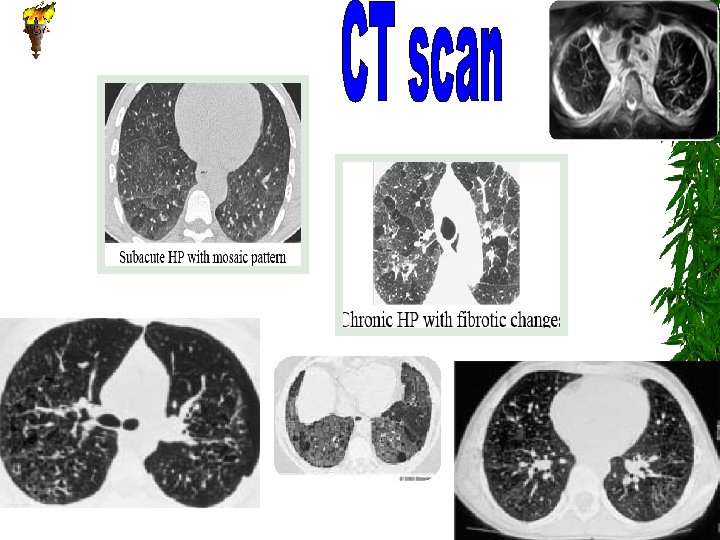
Histologic Classification of ch. ILD DIP Desquamative interstitial pneumonitis CIP Chronic pneumonitisof infancy NSIP Non-specific interstitial pneumonitis FB/LIP OP Follicular bronchiolitis /lymphoid Interstitial Pneumonia Organizing pneumonia (old BOOP) PIG Pulmonary interstitial glycogenosis NEHI Neuroendocrine cell hyperplasia of infancy * UIP: Usual interstitial pneuminitis (rare for children)

Pulmonary Interstitial Glycogenosis
")
Neuroendocrine cell hyperplasia of infancy (NEHI)

DIP CIP Nonspecific interstitial pneumonitis

Follicular bronchiolitis BOOP

Surfactant Metabolism Dysfunction • Surfactant is a complex mixture of phospholipids and proteins (SP-A, -B, -C and -D)& ABCA 3. • ABCA 3 an ATP-binding transporter Of lipids. (ch. ILD) due to ABCA 3 gene mutations

ILD IN CHILDREN Building a diagnostic algorythm BAL Biopsy + Chest Radiogr. + Laboratory Tests BAL PFTs Phys. Exam. PFTs HRCT History HRCT Phys. Exam. Biopsy ? Definitive Diagnosis Chest Radiogr History

ILD IN CHILDREN Treatment ILD with specific cause: • Treatment against underlying disease • Avoidance of triggers ILD of unknown etiology: • Anti-inflammatory medication • Anti-fibrogenic medication • 02 • Supportive care

ILD IN CHILDREN Treatment Anti-inflammatory medication: • Pulsed intravenous methylprednisolone (10 mg/kg/day for 3 days each month) • Oral prednisolone (1 -2 mg/kg/day – taper with response to alternate day regimen)

ILD IN CHILDREN Treatment Anti-fibrogenic medication: • Hydroxychloroquine (6 -10 mg/kg/day in 2 divided doses)
 treatment strategies: • Azathioprine • Cyclophosphamide • Ciclosporin")
ILD IN CHILDREN Treatment Other (experimental) treatment strategies: • Azathioprine • Cyclophosphamide • Ciclosporin • Methotrexate • Lung/heart-lung transplantation

ILD IN CHILDREN Treatment Monitoring of therapy: • • • Resting respiratory rate Exercise tolerance Oxygen saturation Growth/weight assessment PFTs • Chest radiograph • HRCT

ILD IN CHILDREN Outcome Mortality: • All types of chronic ILD: 11% • ILD of unknown etiology: 43% Morbidity: • Poor quality of life: >50% Redding and Fan In Taussig/Landau 1999

ILD IN CHILDREN Directions Areas for future research/collaboration: • Improving histologic classification of paediatric ILD • Searching for alternative concepts for classification • Exploring the genetic background of ILD • Exploring mechanisms of fibrogenesis • Studying new therapeutic concepts in paediatric patients

Download resources Prof Malak Shaheen Lectures
 2011 – pp 55 -79")
ch. ILD review article Vol 5 (1) 2011 – pp 55 -79

Further Readings …. First edition - 2008

Further Readings …. www. childfoundation. info/ch. ILD

Good luck!

Part 2 Pediatric Inhalation Injury By Dr Malak Shaheen

Definition ACUTE Inhalation Injury Acute exposure to high concentrations of toxic gas over a short time CHRONIC Inhalation Injury Low-level continuous or intermittent exposure to irritant gases or chemical vapors

Etiology Accidental or Iatrogenic Why children are vulnerable? are less likely to escape a confined space have a higher minute ventilation (V˚), which increases exposure to smoke and other (i) toxins have relatively smaller airways will be more severely affected by airway edema and obstruction (especially when they have respiratory disease)
 Direct respiratory Cell injury by irritants")
Pathophysiology Inhalation injury occurs in 3 ways: (1) Direct respiratory Cell injury by irritants which cause an inflammatory response, usually from the release of acidic or alkaline radicals. (2) Hypoxemia by interruption of oxygen delivery by asphyxiants. (3)End organ damage by systemic absorption through the respiratory tract by poisons.

Pathophysiology continued Secondary insult with bacterial pneumonia may occur days after inhalation, causing further cytotoxic damage. More water-soluble gases (eg, chlorine, ammonia, sulfur dioxide, hydrogen chloride) dissolve in the upper airway and immediately cause mucous membrane irritation, which arouse alertness early
 Type Irritant gases Inhalant Source Ammonia dyes, plastics, Chlorine Bleaching")
Accidental Inhalation Injury (1) Type Irritant gases Inhalant Source Ammonia dyes, plastics, Chlorine Bleaching agent, disinfectant, Combustion of coal, oil, Combustion of diesel, dyes, Sulfur dioxide Nitrogen dioxide
 Type Inhalant Asphyxiants Carbon monoxide* Hydrogen cyanide† Hydrogen sulfide‡ Source")
Accidental Inhalation Injury (2) Type Inhalant Asphyxiants Carbon monoxide* Hydrogen cyanide† Hydrogen sulfide‡ Source Combustion of weeds, coal, gas, Burning of (silk, nylon, wool) Sewage, volcanic gases, coal mines, natural hot springs * Major component of smoke † Smells like almonds, component of smoke from fires ‡ Smells like rotten eggs
 Type Inhalant Source Systemic Hydrocarbons Inhalant abuse toxins (toluene, benzene,")
Accidental Inhalation Injury (3) Type Inhalant Source Systemic Hydrocarbons Inhalant abuse toxins (toluene, benzene, Freon, glue; gasoline; nail polish remover; kerosene) Organo. Insecticides, nerve phosphates gases Metal fumes/ VAPOR zinc, copper, magnesium, MERCURY (jewelry making)
 inhalation Inhaled Nitric Oxide (i.")
Iatrogenic Inhalation Injury Special Considerations with: Oxygen (O 2) inhalation Inhaled Nitric Oxide (i. NO) Heliox inhalation Hypoxic gases inhalation (Nitrogen, CO 2) Inhalational Anesthetics (N 2 O, Isofluran)
 Hypoxic symptoms Systemic: Neurological Symptoms Cardiac")
Symptoms and Signs Local: Respiratory Symptoms (Upper. Lower) Hypoxic symptoms Systemic: Neurological Symptoms Cardiac Renal Etc…. .

Diagnostic Workup History CXR ABG PFT FOB Xenon V/P scans Spiral CT (is used to evaluate patients with latedeveloping symptoms) Specific tests; Carboxyhemoglobin level, cyanid level ? ? All are qualitative NOT quantitative

Treatment TTT is dependent on type of the inhalation injury. ABCDE Approach 1. 2. 3. 4. Removal from exposure, 24 -h observation (Admit) Supplemental O 2 (except ? ) Drugs; Bronchodilators, inhaled racemic epinephrine, antibiotics, … 5. Advanced respiratory support (? ) 6. Specific Antidote? ? ?

Complications The effect of inhaling irritant gases depends on; The extent and duration of exposure and on the specific agent. Previous chest condition Acute complications: The most serious is ARDS and/or development of bacterial infection.

Prognosis Most children recover fully, but some have chronic complications; Persistent lung injury with reactive airway obstruction &/or Pulmonary fibrosis/ch. ILD;
 Inhalation Injury? Acute and Chronic Inhalation Injury Second")
What about Second Hand Smoke (SHS) Inhalation Injury? Acute and Chronic Inhalation Injury Second hand smoke (SHS) or sidestream smoke (SSS) contains over than 250 toxins and carcinogens Those children usually present with repeated bronchitis, pneumonia, and ear infections.
 www. ersnet. org European Academy of Allergy and")
Free Membership European Respiratory Society (ERS) www. ersnet. org European Academy of Allergy and Clinical Immunology (EAACI) www. eaaci. net

Part 3 Childhood Pulmonary Functions Tests By Dr Malak Shaheen childshaheen@yahoo. com
. John Hutchinson (1811 -1860). The 20 th Century (1850 -1950). Children")
Earliest trial (1681). John Hutchinson (1811 -1860). The 20 th Century (1850 -1950). Children testing (1960 s). Infants and preschool children testing (1980 s).

How to perform PFT in children? Place Child Equipments Operator Reference Values & interpretations (QC)
 Bronchial")
Which Technique? Pediatric PFT Lung Volumes and Ventilation Passive Respiratory Mechanics (Rres &Cres) Bronchial Responsiveness Active Tell me first; What is your clinical Q ? Others
 study (VT, control of")
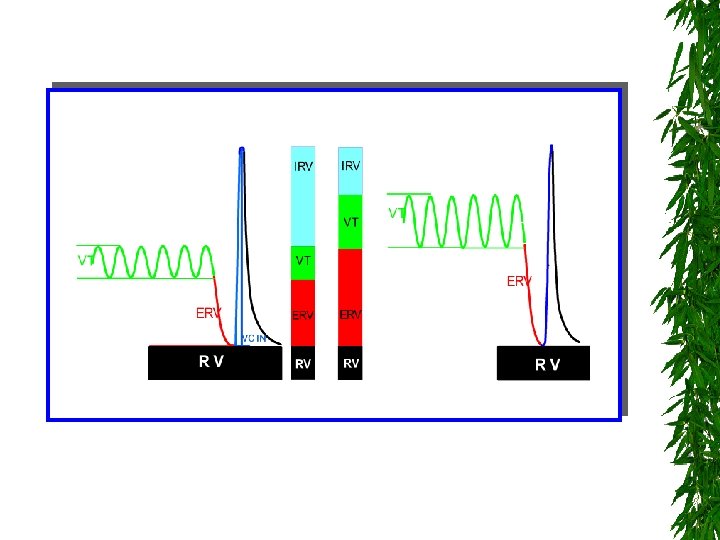
First: Lung volumes and Ventilation Studies 1. Tidal Breathing (TB) study (VT, control of breathing, Tidal flow volume loops) 2. Multiple breath washout (MBWSF 6) test FRC Gas mixing efficiency (LCI)
 - TLC (special circumstances) Master.")
3. Body plethysmography for: - FRC (with tidal breathing) - TLC (special circumstances) Master. Screen body
 A: Passive (Tidal breathing): 1. Plethysmography (Raw &")
Second: Respiratory Mechanics (Rres & Cres) A: Passive (Tidal breathing): 1. Plethysmography (Raw & s. Raw) 2. Occlusion Tech (Rres) 3. Interruption Tech (Rint) 4. Forced oscillation Tech (FOT) (Zres) e. g. IOS
: 1. Spirometry (Special considerations with young children)")
B: Active (Forced Expiratory Tech. ): 1. Spirometry (Special considerations with young children)

How to interpret in children? FEV 1 % Normal Restrictive 80% Mixed Obstructive 80% %FVC Problem: FEV 1 may not be always recorded!

Pediatric Special Notes: Technically acceptable data should not be judged by the duration of the effort (i. e. <1 second). FEVo. 5 and FEV 0. 75 should be calculated and reported in addition to FEV 1 for all children. Even if FEV 1 is there, FEV 1/FVC is more than 90% in the majority of preschool children. Reproducibility criteria of 10% Δ FVC and FEV 1 of best effort is more appropriate for children.
 techniques = squeeze technique -")
2. Partial forced expiratory maneuver Rapid Thoracic Compression (RTC) techniques = squeeze technique - RTC with Tidal breathing (TBRTC) - RTC with external raised volume (RVRTC)
 Which PFT technique? Infant: Tidal RTC")
Third: Bronchial responsiveness (BD, BC and Exercise test) Which PFT technique? Infant: Tidal RTC Preschool child: Rint, FOT, s. Raw School children: Spirometry, Plethysmograph Provocation test? Chemical: both direct (H or M) and indirect (A or H) Physical: cold or dry air Exercise (? )
 using CO (DLco, VA,")
Fourth: Other tests CO Diffusion Test ; Diffusion capacity (DL) using CO (DLco, VA, TLco, Kco) Sa. O 2 ABG Fe. NO PEFM Indirect calorimeter (Canopi test)

PEFM Best PEF X 0. 8 = Lower limit of green Best PEF X 0. 5 = Lower limit of yellow Diurnal Variability: To differentiate between mild intermittent (<20%) and mild persistent (20 -30%) asthma

Pediatric PFTs for different ages Infant Consciousness 1. TB study Sleep/ sedation 3 -6 Y ≥ 6 Y Awake+some Awake+full cooperation √ √ √ √ √ (√) × × √ × √ (rare) √ 7. FOT (Zres) √ 8. Spirometry × √ √ 9. RTC (Partial forced) √ × × 10. Diffusion Test × × √ 2. MBWSF 6 3. Plethysmography (FRC) 4. Occlusion Tech 5. Interruption Tech (Rint) 6. Plethysmography (Raw)

Further Readings Kendig’s Disorders of the Respiratory Tract in Children Seventh Edition 2006
")
Part 4 Pediatric Chest Examination Dr. Malak Shaheen (Ph. D Pediatrics, MSc Critical Medicine)
 3. Investigation")
Pillars of Diagnosis 1. Proper History 2. Clinical Examination (General & Local) 3. Investigation

General Examination Rule of “ 4” 1. 2. 3. 4. ABC D 4 vital data 4 X 2 Skin 4 groups of LN From Head to Toe Rest 4 systems (CVS, Neuro, GIT & Uro)

Local Examination Rule of “ 3” Inspection: 1. Shape 2. Symmetry 3. Respiratory Movement (diagnosis of respiratory distress)

Rule of “ 3” Palpation: 1. Chest expansion 2. TVF 3. Trachea site (Very Important)
: 1. Mid clavicular")
Rule of “ 3” Percussion (Rt & Lf sides in comparison): 1. Mid clavicular line (light) 2. Mid axiliary line (light) 3. Scapular line (heavy)
: 1. Air Entary 2.")
Rule of “ 3” Auscultation(Rt & Lf sides in comparison): 1. Air Entary 2. Breathing sounds 3. Adventitious sounds

Good luck!
- Slides: 77