3 Documentation and Monitoring of Dengue Patients Dengue
















 Fluid")








- Slides: 28
3. Documentation and Monitoring of Dengue Patients Dengue Expert Advisory Group
WHY MONITOR DENGUE PATIENTS? • To differentiate DHF from DF • Assessing onset of Critical Phase of DHF • Smooth manipulation of fluids averting prolonged shock and fluid overload • Early detection of complications • Recognition of unusual presentations
BASIC MONITORING ALL PATIENTS • • • Pulse rate Pulse pressure CRFT Respiratory rate FBC - HCT Intensity of monitoring depends on • Phase of the illness • Severity • Aggressiveness of fluid therapy • Accurate fluid balance charts
Ministry of Health Sri Lanka
FEBRILE PATIENT • Dengue or not? – Clinical – FBC • Leucopaenia + thrombocytopaenia • DF or DHF ? – Plasma leakage + or – • If DHF – what is the phase ?
WHEN PATIENT AFEBRILE • Critical phase – Time of entry – Predicted time of end • • Aggressive monitoring Calculate the fluid quota Dynamic approach to fluid therapy Final diagnosis – precise (DF or DHF & grade)
CRITICAL PHASE FACTS • Dropping Platelets • HCT rise of more than 20% of base line Conforms DHF as it signify leak. Even If HCt rise less than 20% but pleural effusion/ascites present conforms diagnosis of DHF/DSS( it is mostly due to early volume replacement or bleeding).
RECOGNIZE THE STAGE OF THE DISEASE • Febrile phase • Critical phase • Convalescent phase Assess • Day of the illness ? • Evidence of plasma leakage ? • Convalescent rash ?
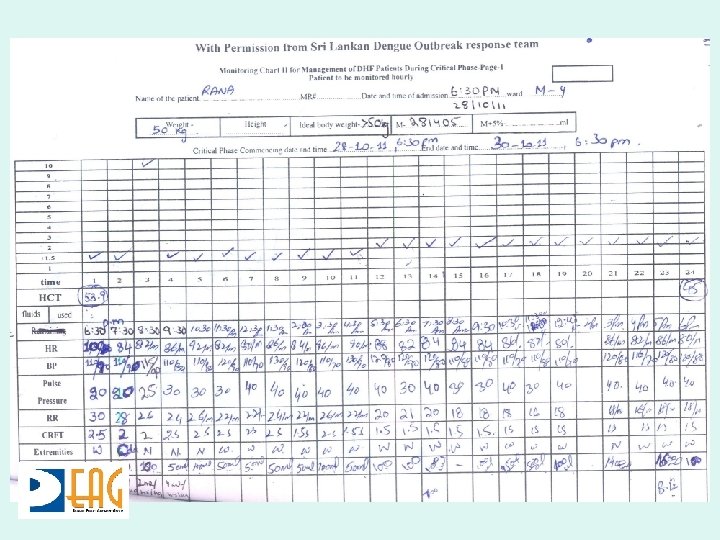
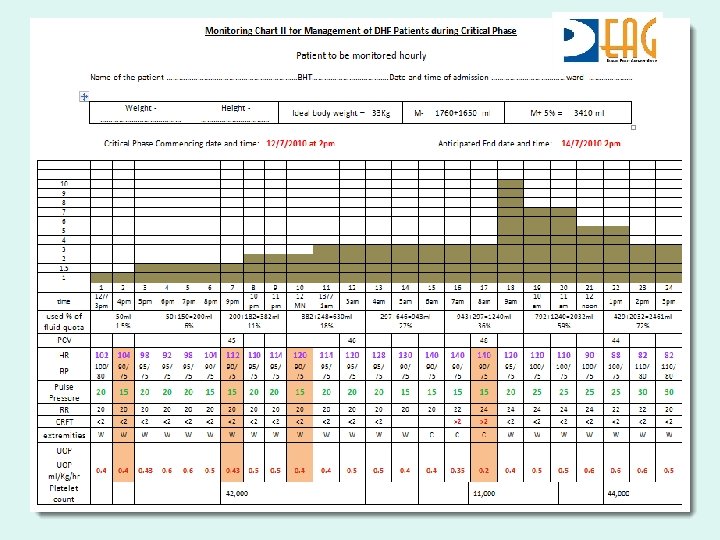
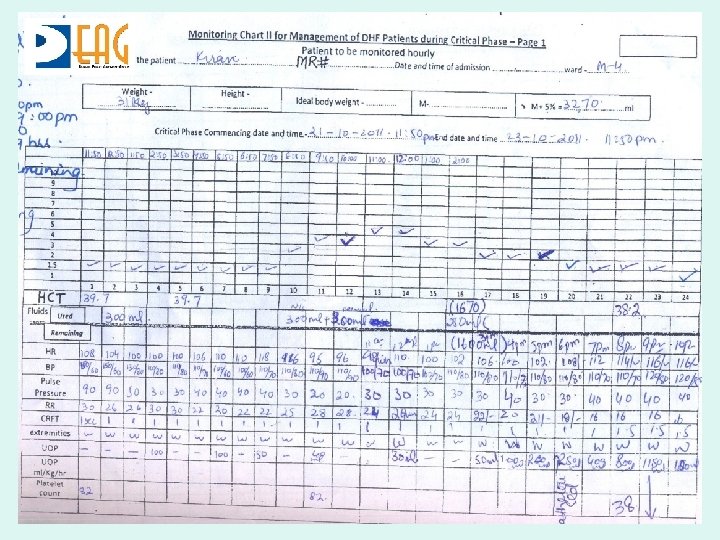
MONITORING & DOCUMENTATION CRITICAL PHASE • Detection of shock • Pulse pressure < 20 mm Hg • CRFT > 2 secs • HCT increase of 20% or more from baseline • Efficacy of IV fluid therapy • Pulse pressure, capillary refill time, hypotension • To keep urine output at least 0. 5 – 1. 0 ml/kg/hr • Early detection of Fluid overload • • Respiratory rate > 20/mt Lung bases Sa. O 2 < 92% CXR
WARNING • Misjudging of critical phase which could begin as early as day 3 (if fever drop on day 3). • Delay in doing the WBC, platelets and Hct determinations. which help predict the critical stage/shock
MONITORING CHART I - FOR MANAGEMENT OF DENGUE PATIENTS – FEBRILE PHASE Hct % e u g n e D Fever D 3 with Fever WBC <5000/mm 3 N-40% L-58% TT + ve D 4 without Fever
Ent r c o t ry in e s a h itical p D 4 with Fever TT + ve, WBC <5000/mm 3 N-40% L 58% Tender Liver
HOW TO TIME THE ONSET OF CRITICAL PHASE? 17 th 8 am 18 th 8 pm 19 th 8 am 19 th 8 pm 20 th 8 am 20 th 8 Pm 21 st 8 am 21 st 8 pm D 3 D 4 D 5 D 6 D 7 WBC 3200 2800 1900 2900 3700 4500 6000 7300 N% 53 41 31 26 25 31 33 43 58 L% 44 56 68 71 73 67 66 55 41 PCV % 39 36 39 42 43 39 44 43 38 Plt 12100 0 11000 61000 0 Onset 22000 18000 12000 8000 End 25200 0 19000
MONITORING IV FLUID THERAPY Phase of the illness – be fully aware • Adequacy of fluid therapy • • • Pulse Pressure >20 mm. Hg CRFT <2 sec Pulse Rate <80/mt UOP > 0. 5 ml/Kg/hr HCT • Early detection of fluid overloading Respiratory rate > 20/mt • Lung bases • Sa. O 2 < 92% • CXR Shift ICU
CLINICAL PARAMETERS General condition Appetite Vomiting Bleeding HCt Urine output (based on IBW) Fluid Therapy PR RR BP/PP Peripheral Perfusion Pulse volume Skin colour Skin Temp. CRFT
CLINICAL SCENARIO • • • If Afebrile Pt. Restless Irritable Pulse rate Pulse volume poor CRFT>2 sec Skin cold Pulse pressure<20 HCT Urine output<0. 5 ml/kg Decision IV Fluid Bolus
SCENARIO • • • Afebrile Restless Confused Decision Pulse volume poor Skin pale CRFT>2 sec Urine output < 0. 5 ml/kg/hr PR BP PP Blood HCt Transfusion
SCENARIO Vital Signs Afebrile patient • Puffy eyelids • Distended abdomen • Tachypnea • Dyspnoea • orthopnea • Respiratory distress • Pulse volume good • Skin colour normal • Skin temp. normal • Pulse pressure • wide • Urine output > 1 ml/kg/hr • CRFT< 2 sec • PR • BP • HCt Decisio n Dextran 40 with frusemide
WARNING • Be vigilant to recognize DSS as most of the patients remain in good conscious and have narrow pulse pressure with increased diastolic pressure(e. g. BP=110/90, 100/80 mm Hg) without hypotension. • Avoid misdiagnosis of DHF in Infants(<1 year) with fits as sepsis/infection followed by LP leading to bleeding/ hematoma(platelets )
PEARLS • Your initial timing of critical phase may prove to be sometimes wrong Be prepared to change what you decided earlier or shift the timing based on more information you receive while Mx.
PEARLS • Try to Master the ways of giving ‘ THE SMOTHEST AND THE MOST UNEVENTFUL RECOVERY’ for the patient. • Avoid both shock and fluid overload. • Keep ‘CHECKING ON A TIME SCALE’… R u heading for fluid overload? If so, switch to a colloid.
PEARLS • At ‘END OF LEAKING PHASE’ even if PCV is high but patient is well, pulse, BP is OK • Don’t try to correct PCV as re absorption will start soon and PCV will come down so. . WAIT.
PEARLS • About 60% of DSS can be successfully resuscitated by using crystalloid solution only, 20% need colloidal and 15% need blood transfusion (+blood components). • With rapid recognition of shock and proper treatment rapid and dramatic recovery is the rule