25 th European Gynecology and Obstetrics Congress 15

25 th European Gynecology and Obstetrics Congress 15 th Ulusal Jinekoloji ve Obstetri Kongresi Current Management of Amenorrhea Münire ERMAN MD Prof Akdeniz University Antalya, TURKIYE

Objective �To define amenorrhea �To review the common causes �Management of amenorrhea �To evaluate the clinical significance
 1. No period by age 13 in the absence of")
Definition Primary Amenorrhea(0. 3%) 1. No period by age 13 in the absence of growth or development of secondary sexual characteristics. 2. No period by age 15 regardless of the presence of normal growth and development with the appearance of secondary sexual characteristics(no menstruation by 4 years after thelarche). ASRM 2008
 In a woman who has been menstruating, the absence of periods")
Definition Secondary Amenorrhea(3%) In a woman who has been menstruating, the absence of periods for a length of time equivalent to a total of at least 3 of the previous cycle intervals or 6 months of amenorrhea
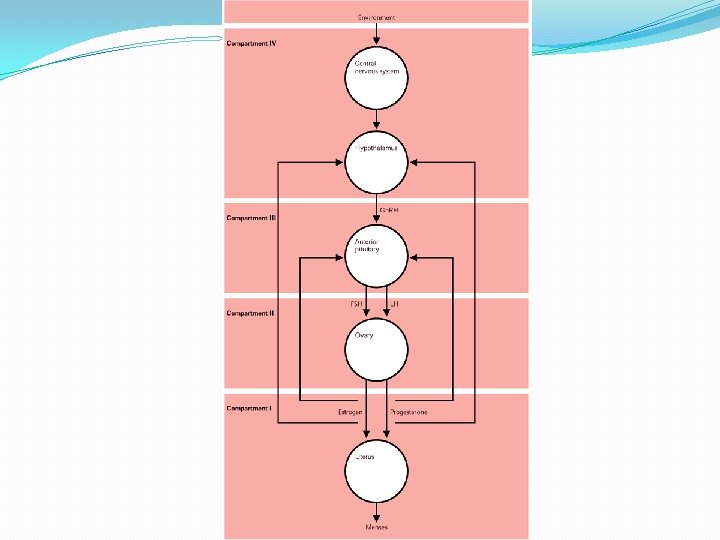

Normal physiology

Most common causes � 1. Policystic ovary syndrome � 2. Hypotalamic amenorrhea � 3. Hyperprolactinemik amenorrhea � 4. Ovarian failure

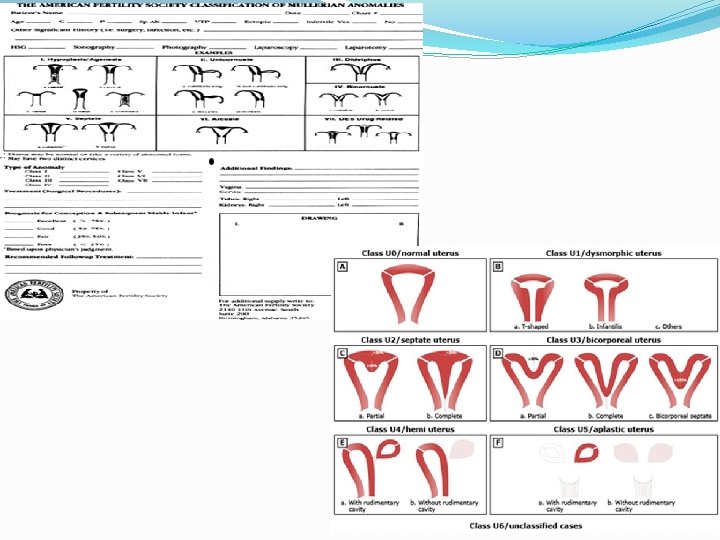
Primary Amenorrhea �Outflow tract anomalies �End organ disorders �Central regulatory disorders

Outflow tract anomalies �Imperforate hymen �Transverse vaginal septum �Vaginal agenesis �Testicular feminization

İmperforate hymen

Transverse vaginal septum �Failure of the Mullerian-derived upper vagina to fuse with the urogenital sinus derived lower vagina.

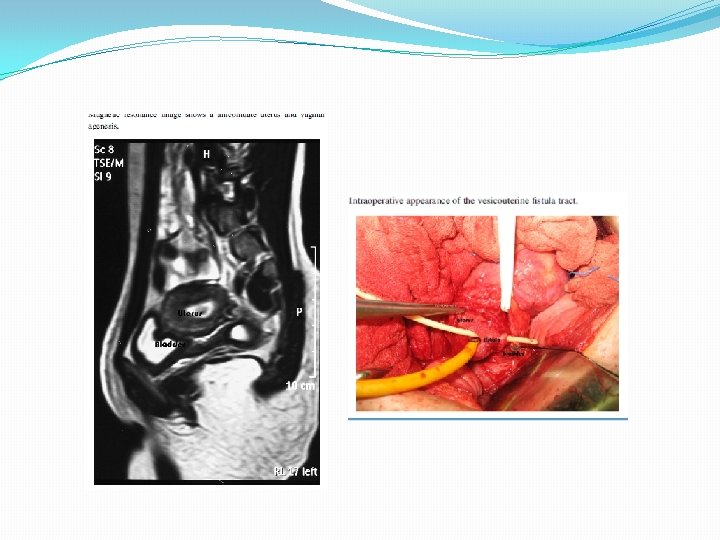
Vaginal agenesis


Sheep grown in the artificial womb Flake et al, 2017, Nature Communications
 Through Ascertainment of a Large Cohort of Families")
�Genetic Analysis of Mayer-Rokitansky-Kuster-Hauser Syndrome (MRKH) Through Ascertainment of a Large Cohort of Families � Fertil Steril 2017, Layman et al

Transmyometrial embryo transfer with Towako catheter
 • 1/50 000 • X-link transmisssion • Testis and")
Testicular feminization (Androgen insensitivity syndrome) • 1/50 000 • X-link transmisssion • Testis and Mullerian inhibiting factor present • Karyotype 46, XY • testosteron level as in male • Treatment: gonadectomy after puberty (HRT) (germ cell malignancy risk? ) • Vaginal reconstruction (dilatation vs Vaginoplasty) • Mongan et al 2015, Best Pract Res Clin Endocrinol Metab. 2015

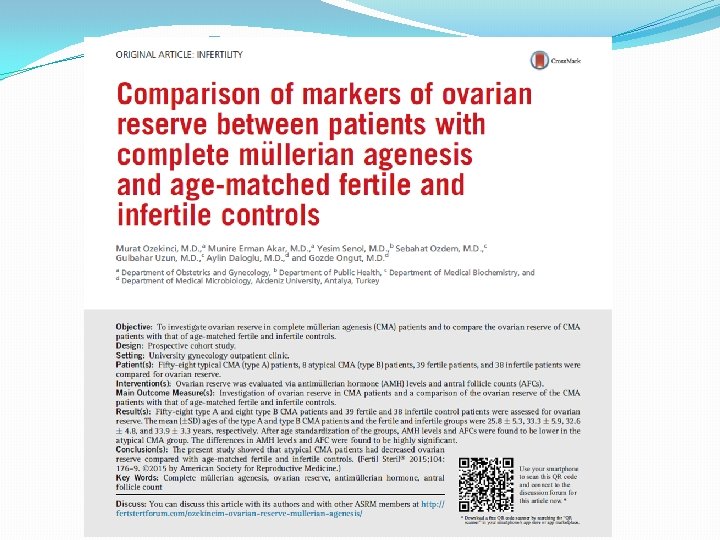
End-Organ Disorders �Ovarian failure �Gonadal agenesis with 46 XY chromosome

Ovarian failure �Hypergonadotropic hypogonadism �İdiopathic �Steroidogenic enzyme defects � Cholesterol side chain cleavage � 17 hydroxylase � 17 desmolase �Pure gonadal dysgenesis (Swyer syndrome) �Turner syndrome �Savage syndrome � Mc Cabe , 2014, Pediatr Endocrinol Rev

Turner syndrome Levitsky et al 2015, Curr Opin Endocrinol Diabetes Obes
 �Primary amenorrhea �tall stature, lack of secondary sexual characteristics")
Swyer syndrome (XY gonadal dysgenesis) �Primary amenorrhea �tall stature, lack of secondary sexual characteristics development �female external genitalia, normal vagina and fallopian tubes �hypoplastic uterus, and streak gonads. �Mutation in SRY gene (sex determining region of Y chromosome) � 1955, Swyer et al

Fertil Steril 2011

Central disorders �Hypothalamic disorders �Pituitary disorders �Adrenal disorders

Hypothalamic dysorders �Hypothalamus unable to produce Gn. RH �Anovulation and amenorrhea �Kallman syndrome (migration of the Gn. RH neurons are disrupted from olfactory placode to hypothalamus) �Tumor mass effect �Trauma �Sarcoidosis �Tuberculosis �Irradiation �Anorexia nervosa �Hyperprolactinemia �Hypothyroidism

Pituitary dysorders �Tumors �Infiltration of the pituitary �İnfarct of the pituitary �Hemosiderosis
")
21 hydroxylase deficiency (Late onset CAH)

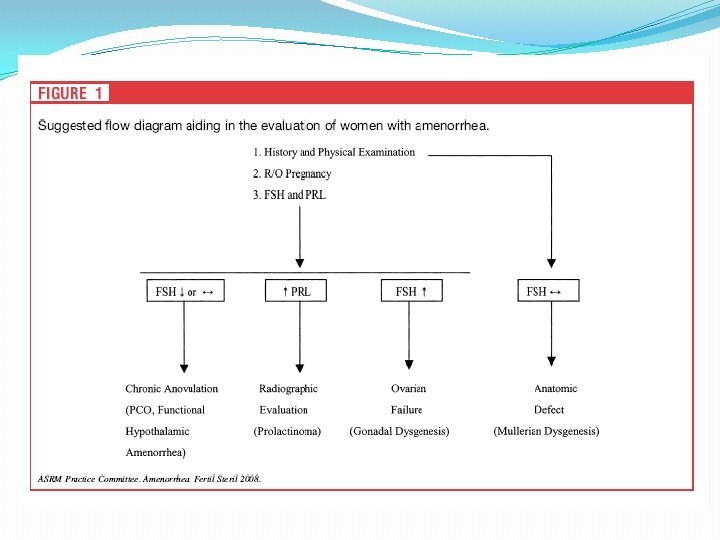
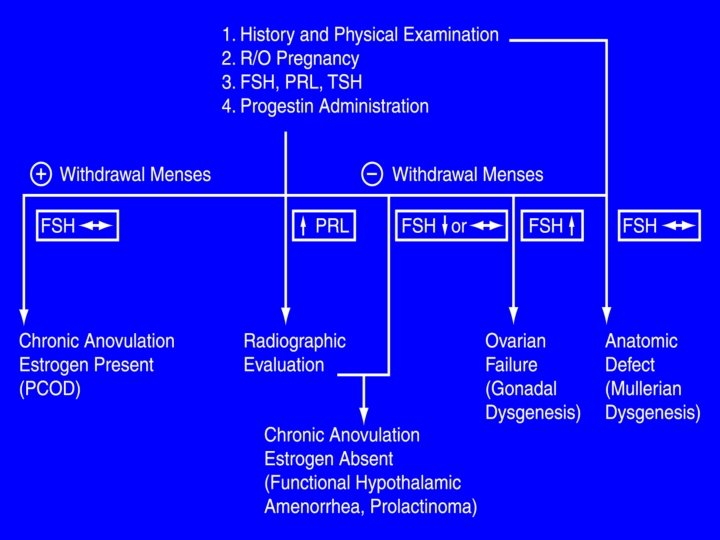
Evaluation of the patient �History �Physical examination �Breast development �Presence of hirsutizm, virilization �ßh. CG �FSH �TSH �Prolactin

Uterus absent Uterus present Breasts absent Gonadal agenesis in 46 XY Gonadal failure/agenesis in 46 XX Breasts present Enzyme deficiencies in testesterone synthesis Disruption of hypothalamic pituitary axis Testicular feminization Hypothalamic, pituitary or ovarian pathogenesis Mullerian agenesis Congenital abnormalities of the genital tract Lobo et al, 2007 Fertil Steril
 Acc to the presence of secondary sexual characteristics in")
Primary amenorrhea(Katz 2007, Lobo R) Acc to the presence of secondary sexual characteristics in 4 categories 1. No breast develop, presence of uterus 2. Presence of breast develop, no uterus 3. No breast development, no uterus 4. Presence of breast development and uterus
Gonadal failure �B)Hypothalamic failure due to insuff Gn.")
1. No breast development, uterus present �A)Gonadal failure �B)Hypothalamic failure due to insuff Gn. RH �C)Pituitary failure
Androgen insensitivity(testicular feminization) �B)congenital agenesis of uterus")
2. Breast development, no uterus �A)Androgen insensitivity(testicular feminization) �B)congenital agenesis of uterus
 Normal breast develop No sexual")
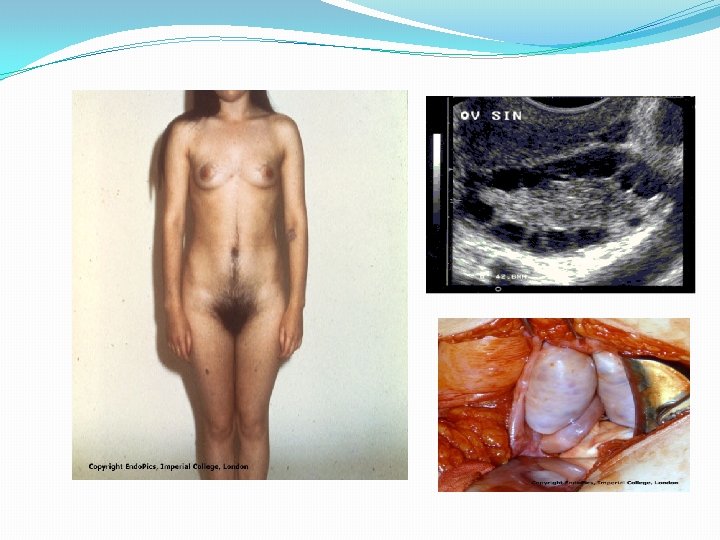
Karyotype 46 -XY 46 -XX Androgen Insensitivity (TSF syndrome) Normal breast develop No sexual hair Mullerian Agenezis (MRKH syndrome) Normal breast d evelopment and sexual hair
17 -20 desmolase def �B)agonadizm")
3. No breast development and no uterus �A)17 -20 desmolase def �B)agonadizm
Hypotalamic etiology �B)Pituitary etiology �C)Ovarian etiology �D)Uterine")
4. Breast development and presence of uterus �A)Hypotalamic etiology �B)Pituitary etiology �C)Ovarian etiology �D)Uterine etiology

Asherman’s Syndrome

Amenorrhea+ Hyperandrojenemia Testosteron, DHEAS, FSH and LH TEST. >200 ng/d. L DHEAS >700 mg/d. L Serum 17 -OH Progesterone levels U/S ? MRI or CT varian or adrenal tumor DHEAS 500 -700 mg/d. L Adrenal hyperfunction Late CAH Mildly high DHEAS PCOS (inc LH / FSH)

General principles in management. Restoration of ovulatory function �If not possible HRT and prevention of osteoporosis and atherosclerosis �Progesteron for prevention of endometrial hyperplasia in patients with normal estradiol levels �Vaginal reconstruction in vaginal agenesis �If there is Y chromozome gonadectomy following puberty � (52%) risk of gonadoblastom, disgerminom, and yolk sac tumors

SUMMARY �Most common causes � 1. Policystic ovary syndrome � 2. Hypotalamik amenorhea � 3. Hyperprolactinemik amenorhea � 4. Ovarian failure �First lab tests ßh. CG, FSH, TSH and prolaktin
- Slides: 47