2003 n300 000 Stage I 24 Stage IV



 Stage I 24% Stage IV 22% Stage II 26% Stage")


 615( 1980) 703( 1980) 123( 1982)")
 1370( 1984) 495( 1980) 1061(")




 significant p-value? Absolute gain (%)")






 Survival GISTG 7175")
 50. 4 Gy CI 5 -Fu Surg 5 -Fu x 4 Surg")
 5 -Y preop(%) postop(%) P complete RT 92 54 <0. 001")




- Slides: 81
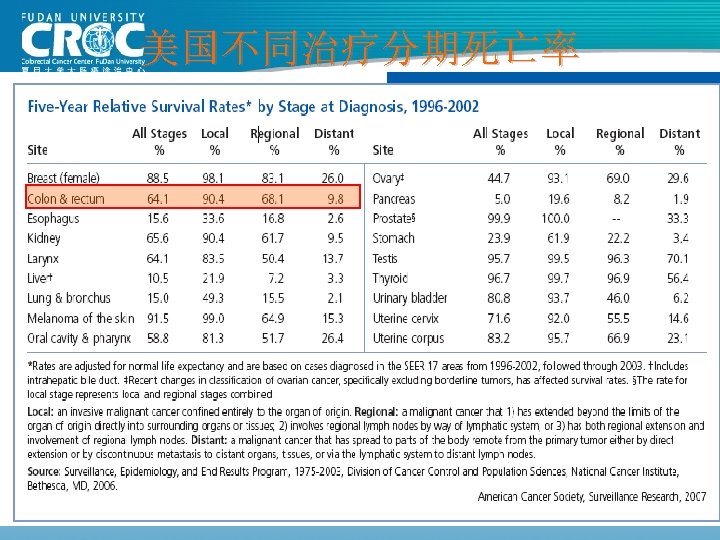
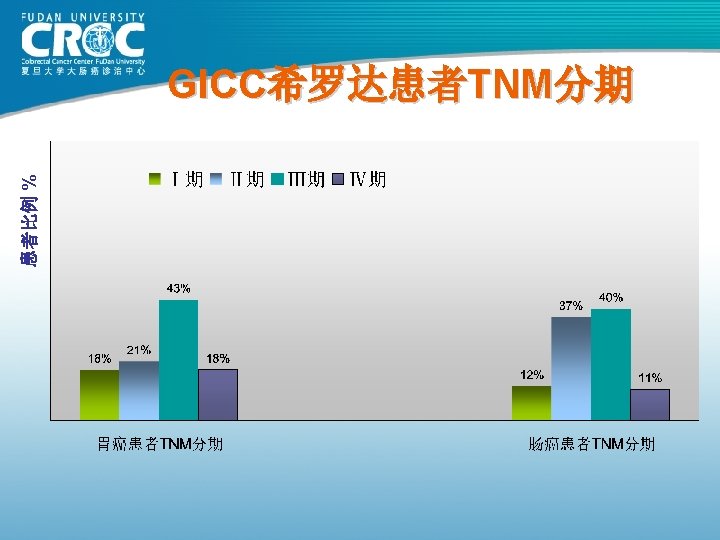
美国和西欧大肠癌发病分期 2003 (n≈300, 000) Stage I 24% Stage IV 22% Stage II 26% Stage III 29%
上海市大肠癌生存分析 市区 一年 885 68. 25 观察生存率% 二年 三年 四年 57. 40 49. 38 45. 31 五年 42. 03 中位生存期 天 月 1067 36 郊区 602 67. 11 54. 98 50. 00 45. 85 43. 02 1095 37 56. 42 55. 48 60. 10 57. 40 62. 28 60. 34 61. 39 65. 97 64. 49 65. 26 49. 63 48. 10 53. 63 50. 40 52. 97 51. 50 52. 29 58. 94 58. 16 58. 56 45. 53 43. 48 50. 24 46. 30 47. 51 47. 56 47. 53 52. 66 53. 06 52. 85 42. 43 40. 60 47. 98 43. 67 43. 50 43. 98 43. 72 50. 00 50. 61 50. 30 1075 1001 1499 1131 1294 1234 1271 1825 - 36 33 50 38 43 41 42 61 - 瘤别 性别 地区 结肠癌 男性 女性 直肠癌 男性 女性 2002 全市 市区 郊区 全市 病例数 1487 867 619 1486 623 532 1155 526 490 1016 67. 79 67. 94 71. 24 69. 31 74. 16 74. 44 74. 29 77. 19 76. 33 76. 77 上海CDC 2008
80年代结肠癌手术疗效 Monash MSKCC 杭州肿瘤 上海瑞金 上海肿瘤 例数 (年份) 615( 1980) 703( 1980) 123( 1982) 302( 1983) 261( 1985) Dukes’A 88 69. 25 62. 09 100 93. 25 Dukes’B 78 69. 25 62. 09 74. 74 82. 70 Dukes’C 60 52. 19 38. 92 C 1: 45. 18 C 2: 28. 44 73. 62 75. 9 61. 82 72. 79 83. 84 5年生存率 76 (%)
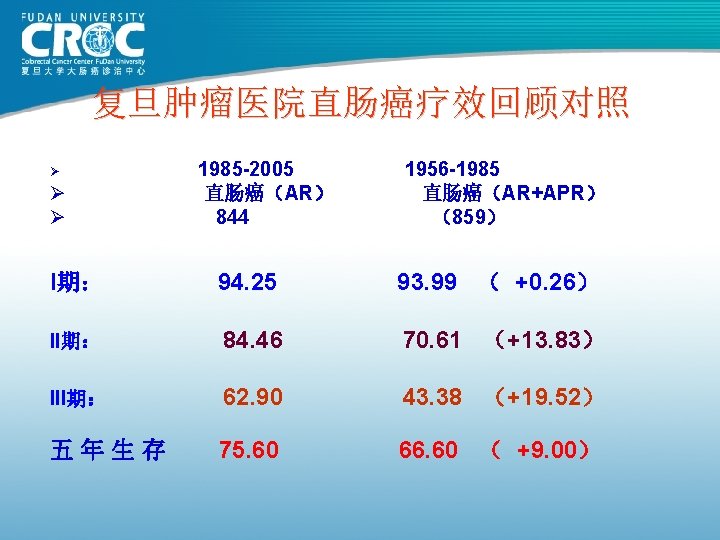
80年代直肠癌手术疗效 St. Mark’s MSKCC Monash 上海瑞金 上海肿瘤 例数 (年份) 1370( 1984) 495( 1980) 1061( 1980) 619( 1983) 859( 1985) Dukes’A 85. 6 77 88 98. 05 93. 99 Dukes’B 67. 5 77 76 68. 43 70. 61 Dukes’C 41. 3 41 41 C 1: 39. 66 C 2: 10. 21 43. 38 63 69 66. 91 66. 6 5年生存率 (%)
2007 恶性肿瘤治愈方式 Ø 60% are cured by surgery alone Ø 10% are cured by radiotherapy alone Ø 4% are cured by chemotherapy alone Ø 26% are cured by the combination of surgery, radiotherapy and/or chemotherapy
英国恶性肿瘤处理 The Law says 2007 Ø All patients with possible cancer MUST be seen by a specialist within 2 weeks of presentation to their family doctor (General Practitioner) Ø All diagnostic investigations MUST be completed with 4 weeks Ø All patients with a confirmed diagnosis of cancer MUST be discussed by the appropriate Multi-Disciplinary Team before treatment commences Ø Treatment MUST commence within 31 days of the confirmed diagnosis of cancer
II期患者辅助治疗:反对意见 Ø INT-00351 Ø IMPACT B 22 Ø ASCO meta-analysis 3 1. Moertel CG et al. J Clin Oncol 1995; 13: 2936– 43 2. IMPACT B 2 Investigators. J Clin Oncol 1999; 17: 1356– 63 3. Benson et al. J Clin Oncol 2004; 22: 3408– 19
II期结肠癌辅助治疗: 研究数据 Trials analysed n Relative risk reduction (%) significant p-value? Absolute gain (%) INT-0035 1 318 31 no 8 IMPACT-B 2 5 1 016 17 no 3 ASCO-B 2 12 3 732 14 no - NSABP 4 1 564 30 - - Netherlands 1 468 19* - - CKVO 1 460 26* - 8 QUASAR-1 1 3 238 22 yes 4 Japan 3 2 295 22 no 5 MOSAIC 1 576 24† - 5 *OS; †high-risk patients
辅助治疗的生存优势: 20, 898 例病患的证据 Stage II 8 -year OS Stage III 8 -year OS 1. 0 ∆=5. 4% p=0. 026 0. 8 0. 6 0. 4 Surgery alone: 66. 8% 0. 2 0 1 2 3 4 5 Surgery alone: 42. 7% 0. 2 Surgery + FU-based chemotherapy: 72. 2% 0. 0 ∆=10. 3% p<0. 0001 Surgery + FU-based chemotherapy: 53. 0% 0. 0 6 7 8 0 1 2 3 4 5 6 7 8 Follow-up (years) Sargent et al. JCO 2009
� 助 放 化 � 的 � 后 Series Local failure(%) Survival GISTG 7175 11 54% (8 -years) 79 -47 -51 14 53% (5 -years) 86 -47 -51 9 -11 60 -70% (4 -years) INT 0114 9 -13 78 -80% (3 -years) 8 62 -65% (5 -years) NSABP R-02
CAO/ARO/AIO 94(德国研究) 50. 4 Gy CI 5 -Fu Surg 5 -Fu x 4 Surg 50. 4 Gy CI 5 -Fu x 4 T 3 NEJM,351: 1731 -1740,2004
CAO/ARO/AIO 94 (德国研究) 5 -Y preop(%) postop(%) P complete RT 92 54 <0. 001 Complete CT 89 50 <0. 001 3 -4 acute toxicity 27 40 0. 001 3 -4 late toxicity 14 24 0. 01 p. CR 8 0 <0. 001 SP 39 19 0. 004 LF 6 13 0. 006 DM 36 38 0. 84 DFS 65 68 0. 80 OS 74 76 0. 32
新�助放化�治��果 Results EORTC FFCD Polish German 急性毒刑反应 54% 15% 18% 27% 完全有效 13. 7% 11. 7% 16% 8% 保肛率 55% 53% 58% 69% 局部复发率 8. 7% 8% - 6% 总生存率 65% 67% - 74% Lisa M ASCO 2005
肝转移治疗现状及展望 80– 85% unresectable 10– 15% resectable CT RR ~40 -70%1, 2, 3 32– 80% not resectable after single agent in 1 st line Resection 30%? 2, 3 Triplet therapy Doublet + biologic?