18 th NOCR Meeting Las Vegas Nevada February

18 th NOCR Meeting Las Vegas, Nevada – February 2012 An Update in Chronic Myeloid Leukemia (CML): The Clever ‘Stupid Cancer’ David Steensma, MD FACP Associate Professor of Medicine, Harvard Medical School Adult Leukemia Program, Dana-Farber Cancer Institute

CML: a disease of “firsts” • 1845 – first clear description of leukemia • 1960/1972 – first association of a recurrent chromosomal abnormality (“Philadelphia chromosome”) with cancer… and second to be recognized as a reciprocal translocation (t(9; 22), found after t(8; 21)) • 1982 – first fusion protein associated with cancer (BCR/ABL) David Craigie John Hughes Bennett Peter Nowell and David Hungerford Annalies de Klein Nora Heisterkamp Rudolf Virchow Janet Rowley John Groffen • 1999 – first tyrosine kinase inhibitor with clinical activity against a fusion protein (CGP 57148 b=STI 571=imatinib) Brian Druker • 2000 – first description of “Darwinian” emergence of molecular resistance to a targeted agent (e. g. , T 315 I ABL mutation) Imatinib

Survival in early chronic phase CML Year Imatinib era 1990 -2000 1982 -1989 1975 -1981 1965 -1974 1. 0 Proportion surviving 95% 0. 8 Total 230 960 365 132 123 Dead 7 334 265 127 122 0. 6 Interferon α, cytarabine, allogeneic stem cell transplant 0. 4 0. 2 0 0 2 4 6 8 Years from referral 10 12 Hydroxyurea, busulfan, splenectomy 14

What to expect with current therapies
 in imatinib arm")
IRIS Phase III trial of imatinib vs. cytarabine/interferon: overall survival (ITT) in imatinib arm 100 90 80 Alive, % 70 Estimated overall survival at 8 years was 85% (93%, considering only CML-related deaths) 60 50 40 30 Survival, deaths associated with CML 20 Overall Survival 10 0 0 12 24 36 48 60 Months Since Randomization 72 84 ITT: intent-to-treat; OS: overall survival O’Brien SG, et al. American Society of Hematology annual meeting 2009. Abstract 1126. 96 108

IRIS Study: imatinib patient status at 60 months Continued Imatinib 3% 11% 4% Withdrew consent Death 3% 3% Protocol violation 2% SCT 5% Adverse Event 69% Crossed over to IFN Cumulative failure rate ~30% Unsatisfactory therapeutic effect Druker B et al. NEJM 2006 355: 23, 2408 -17

Risk assessment in CML Study Calculation Risk Definition Sokal et al, 1984 Exp 0. 0116 x (age in years – 43. 4) + (spleen in cm – 7. 51) + 0. 188 x [(platelet count / 700)2 - 0. 563] + 0. 0887 x (blast cells – 2. 10) Low: <0. 8 Intermediate: 0. 8 -1. 2 High: >1. 2 Hasford et al, 1998 0. 666 when age ≥ 50 years + (0. 042 x spleen in cm) + 1. 0956 when platelet count >1500 x 109/L + (0. 0584 x blast cells) + 0. 20399 when basophils >3% + (0. 0413 x %eosinophils) x 100 Low: ≤ 780 Intermediate: 781 -1480 High: >1480 http: //www. icsg. unibo. it/rrcalc. asp http: //www. leukemia-net. org/content/leukemias/cml_score/ Sokal JE et al, Blood 1984; 63: 789 -799 Hasford J et al, J Nat Cancer Inst 1998; 90: 850 -858

Are patients ever cured with TKIs?

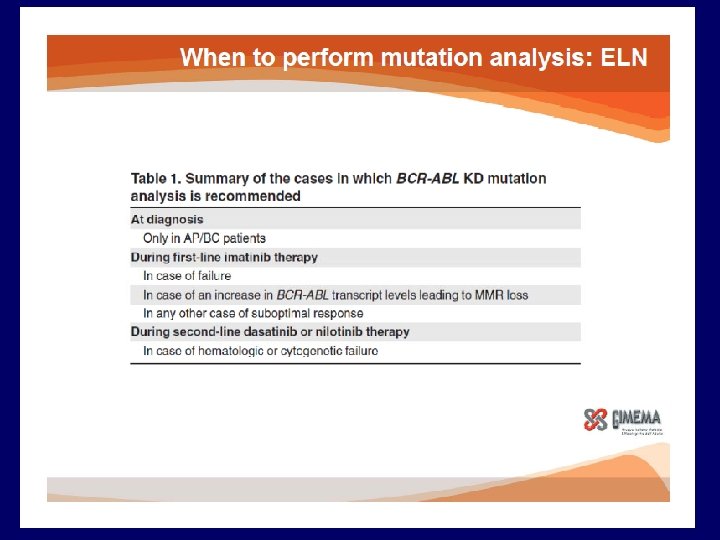
When should mutation testing be done?
 De novo CP CML 58")
Factor Analyzed N N positive for KD mutation (%) De novo CP CML 58 1 (2%) De novo AP/BC CML 12 2 (17%) IM Failure (ELN criteria) 166 45 (27%) Suboptimal IM Response (ELN) 233 11 (5%) Rise in PCR without loss of MMR 70 0 (0%) Rise in PCR with loss of MMR 89 4 (5%) NIL/DAS ‘Failure’ (ELN criteria) 19 11 (58%) NIL/DAS ‘Suboptimal’ (ELN criteria) 19 4 (21%)

Treatment options based on BCR-ABL kinase domain mutation status Mutation Treatment recommendation T 315 I Stem cell transplant or clinical trial (e. g. , ponatinib, omacetaxine) V 299 L, T 315 A, F 317 L/V/I/C Consider nilotinib; likely resistant to dasatinib Y 253 H, E 255 K/V, F 359 V/C/I Consider dasatinib; likely resistant to nilotinib Any other mutation Unclear; consider high-dose imatinib, nilotinib, dasatinib Based on NCCN and ELN guidelines (Soverini S et al Blood 2011)

Does early molecular response matter?
 and")
Molecular and Cytogenetic Response at 3 Months of Imatinib Predicts Progression-free Survival (PFS) and Overall Survival (OS) – a Follow-Up Analysis of the Randomized CML-Study IV Benjamin Hanfstein, MD, Martin C. Müller, MD, Philipp Erben, MD, Michael Lauseker, Susanne Saussele, MD, Ulrike Proetel, MD, Susanne Schnittger, Ph. D, Claudia Haferlach, MD, Hans-Jochem Kolb, MD, Stefan W. Krause, MD, Christoph Nerl, MD, Dominik Heim, MD, Gabriela M. Baerlocher, MD, Jörg E. A. Schubert, MD, Hermann Einsele, MD, Mathias Hänel, MD, Jolanta Dengler, MD, Christiane Falge, MD, Lothar Kanz, MD, Andreas Neubauer, MD, Michael Kneba, MD, Frank Stegelmann, MD, Michael Pfreundschuh, MD, Cornelius F. Waller, MD, Markus Pfirrmann, Ph. D, Jörg Hasford, MD, Wolf-Karsten Hofmann, MD, Rüdiger Hehlmann, MD, Andreas Hochhaus, MD, for The SAKK and for The German CML Study Group
 §")
Patients and samples § N = 1, 223 (assigned by April 30, 2010) § Median age 52 years (16 -85), 39% female § Median observation time 4. 8 years § Treatment: § Imatinib 400 mg/d n = 335 (27%) § Imatinib 400 mg/d + Interferon alpha n = 366 (30%) § Imatinib + Cytarabine n = 149 (12%) § Imatinib 800 mg/d n = 373 (30%)
 BCR-ABL IS at 3 months ≤ 10% vs. >10% ≤ 10%")
Progression-free Survival (PFS) BCR-ABL IS at 3 months ≤ 10% vs. >10% ≤ 10% >10% BCR-ABLIS n 5 Y-PFS ≤ 10% 499 93% >10% 189 87% p-value 0. 003
 BCR-ABLIS at 3 months ≤ 10% vs. >10%")
Overall Survival (OS) BCR-ABLIS at 3 months ≤ 10% vs. >10%

What’s coming…

Some practical tips

What is needed at initial diagnosis? • CBC+differential; complete metabolic profile including liver tests • Bone Marrow Aspirate and Biopsy – Cytogenetics (20 metaphases) – ? FISH, ? QPCR • Why is a bone marrow necessary? – Need to exclude AP/BP-CML. – Sokal/Hasford score predictive of response to TKIs – Helpful to review entire karyotype (useful for comparison at time of relapse) – FISH important for “cytogenetic negative” CML (<5%) – FISH may have some role in prognosis, e. g. , del 9 q+ NCCN Guidelines 2012

How do I choose initial therapy? • Imatinib at 400 mg daily remains the ‘standard of care’ – But it will fail ~30% of patients – And it is rarely curative • However, reasonable to choose a 2 nd Generation TKI: – Especially for higher-risk disease based on Sokal or Hasford scores – Young patient, as 2 nd generation TKI best chance of obtaining CMR and MMR, and reduces progression to AP/BP – Nilotinib and dasatinib likely very similar, and differences largely from different trial designs and/or locations; choose based on adverse event profile NCCN Guidelines 2011.

How to follow your patient? • • • CBC+differential, complete metabolic profile – Every 3 months; maybe more frequent earlier on Bone Marrow Aspirate and Biopsy with Cytogenetics (20 metaphases) – Every 6 months until Complete Cytogenetic Remission (CCR) – Further bone marrow exams PRN Quantitative RT-PCR – Every 3 months indefinitely – Can go to every 6 months, after 2 years of major molecular response – FISH not as helpful • Only follow in patients with cytogenetic negative CML (<5%) NCCN Guidelines 2012

Pearls • Maximize patient adherence by managing adverse events “The most important cell in CML resistance is the neuron” “Once disease is in advanced phase, the game is largely over” – Never dose reduce imatinib below 300 mg daily or nilotinib below 400 mg daily or dasatinib below 50 mg daily – Heme toxicities (ANC < 1000; Plts < 75 K): rare, usually early, and easily managed • Never change dose or therapy based solely on a single PCR – Repeat in 1 month – Confirm with bone marrow exam before changing therapy • Mutational Analysis – Not useful at initial diagnosis or in responding patients – Send at time of any change in therapy (increase in dose or 2 nd TKI) • Stem Cell Transplant – Refer at time of 1 st failure (want to know donor status) – Refer to transplant in patients who fail 2 nd TKI, have a T 315 I or AP/BP-CML

Thank you!
- Slides: 25