16 th Conference on Retroviruses and Opportunistic Infections

 1003 Abstracts")







 System")


")

")








 < 50 HVI-1 RNA copies")

 q Pr. EP")

 PI 23")
- Slides: 30
16 th Conference on Retroviruses and Opportunistic Infections February 8 -11, 2009 Palais des Congrès de Montréal, Canada Javier Martinez-Picado
HIV Drug Resistance 61 abstracts (6, 1%) 1003 Abstracts
HIV Drug Resistance Oral Sessions: 18. Mechanisms of Drug Resistance and Optimal Timing of ART (9) 32. HIV Drug Resistance and Treatment Response (4) Poster Sessions: 114. Evolution of RT and PI Resistance in Patients (9) 115. Drug Resistance and Viral Fitness (4) 116. Outcomes of HIV Drug Resistance (11) 117. Circulating Drug Resistance in HIV-infected Populations (6) 118. Transmission of Drug-resistant HIV (7) 119. Use of Novel Technologies to Understand HIV Drug Resistance (7) 120. Resistance Assays and Their Imterpretation (4)
Mechanisms of Drug Resistance
Mechanisms of Resistance to RT inhibitors N 348 I in HIV-1 RT counteracts the antagonism between TAMs and Y 181 C (Abstract 68) AZT + NVP antagonistic interaction between TAMs and Y 181 C Treatment efficacy AZT + NVP These patients were 2. 6 times more likely to acquire pol 1 318 -9 426 -7 560 connection RNase H 8 I Current 1 genotyping 250 N 348 I N 3 4 N 348 I in the connection domain of HIV-1 RT N 348 I is highly associated with TAMs and Y 181 C Nikolenko, PNAS 2007; Yap, PLo. S Med. 2007; Delviks-Frankenberry, PNAS 2008; Ehteshami, J Biol Chem. 2008; Hachiya, J Virol. 2008
Mechanisms of Resistance to RT inhibitors N 348 I in HIV-1 RT counteracts the antagonism between TAMs and Y 181 C (Abstract 68) Biochemical and cell-based assays demonstrate that N 348 I restores AZT-resistance phenotype AZT-resistance AZT resentization TAM (AZT) N 348 I (AZT/NVP) Y 181 C (NVP)
Evolution of RT and PI Resistance in Patients
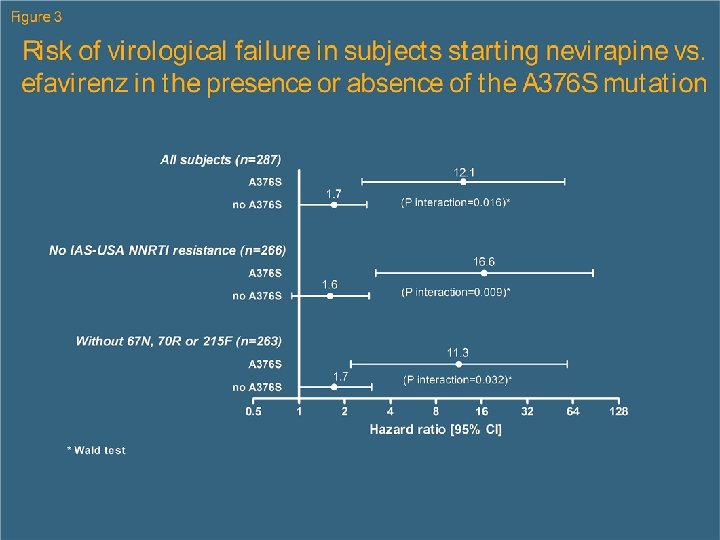
Evolution of RT and PI Resistance in Patients Polymorphism A 376 S in the Connection Domain (Abst. 646) 1 q q 426 -7 76 S pol 318 -9 560 connection RNase H 250 N 348 I A 3 Current 1 genotyping Present in approx. 5% of the naïve patients Increases up to 15% in ARV-experienced patients Associated with NVP failure No association with other Drug Resistance Mutations
Use of Novel Technologies to Understand HIV Drug Resistance variants
Use of Novel Technologies Ultra-deep Sequencing (Abst. 124, 125, 679, 680, 682, 683) System throughput/8 h = 1 Gb Total clonal reads > 2, 000 Read length = 400 bp Cost = $10, 000
1. Emulsion Based Clonal Amplification A + PCR Reagents + Emulsion Oil B Micro-reactors Adapter carrying library DNA Mix DNA Library & capture beads (limited dilution) “Break micro-reactors” Isolate DNA containing beads Create “Water-in-oil” emulsion Perform emulsion PCR • Generation of millions of clonally amplified sequencing templates on each bead • No cloning and colony picking
2. Depositing DNA Beads into the Pico. Titer™Plate Load beads into Pico. Titer™Plate Load Enzyme Beads Centrifuge Step 44 μm 1. 6 million wells
3. Sequencing by Synthesis (Pyro. Sequencing)
4. Biocomputational analysis
Use of Novel Technologies Ultra-deep Sequencing q Quantification of tropism (Abst. 124, 679, 680) § Detecting minority virus: ü Broad distribution of prevalence of X 4 variants in clinical isolates that are not detected by standard sequencing techniques § Implications for ART: ü Initially minority variants can increase in frequency in a matter of days due to drug pressure ü A low prevalence of X 4 was associated with improved virological response to Maraviroc, even when standard Trofile indicated DM or X 4 virus
HIV Drug Resistance variants and Treatment Response
HIV Drug Resistance and Treatment Response Emerging Patterns of Resistance to Integrase Inhibitors (Abst. 125) q Resistance data from 5 clinical studies are generally consistent: § 3 studies in treatment-experienced patients and 2 in treatment-naïve patients q Three pathways primary mut Y 143 C/H/R, Q 148 H/K/R, N 155 H q Secondary mutations lead to higher resistance § If not present at VF, evolves at later time q Q 148 pathway is preferred § Virus population can switch N 155 to Q 148 § When combined with secondary mut, Q 148 mutants lead to greater resistance
HIV Drug Resistance and Treatment Response Emerging Patterns of Resistance to Integrase Inhibitors (Abst. 125) q RAL resistance-associated mutations (RAMs): § No primary RAL RAMs (i. e. , 143, 148, 155) detected at baseline, consistent with previously published data by: Buzón et al. Raltegravir susceptibility and fitness progression of HIV type-1 integrase in patients on longterm antiretroviral therapy. Antivir Ther. 2008; 13: 881 -93 § Secondary RAL RAMs (L 74 M, E 92 Q, T 97 A, E 138 A/K, G 140 A/S): only T 97 A observed at baseline; frequency not significantly different between patients with and without virologic failure q Polymorphisms § 25 of 28 baseline polymorphisms analyzed to date had no significant difference in frequency between virologic failures and treatment successes (exceptions: S 17 N, M 50 I, and D 256 E)--Further data needed to confirm
HIV Drug Resistance and Treatment Response Emerging Patterns of Resistance to Integrase Inhibitors (Abst. 125, 685) q Minority variants § Primary RAL RAMs were detected at exceedingly low frequencies in baseline samples ü None detected by ultra-deep sequencing (LOQ = 0. 4%) ü Frequencies of <0. 2% were detected by PASS § Primary RAL RAMs detected by PASS at baseline did not emerge in any patients who experienced virologic failure § Primary RAL RAMs appearing during PN 004 monotherapy were rare, occurred at low levels, and did not result in virologic failure during the combination therapy phase
Circulating Drug Resistance in HIV-infected Populations
Circulating Drug Resistance Lack of drug resistance monitoring is associated with an increased risk of mortality (Abst. 666) q Clinical and demographic factor associated with failing to receive HIV drug resistance testing when indicated q Association between access to resistance testing before and after starting HAART and mortality. q 1820 participants that initiated HAART between Jan’ 00 and Jun’ 06 and were followed until Jun’ 07 in an environment with universal free access to health services.
Circulating Drug Resistance Lack of drug resistance monitoring is associated with an increased risk of mortality (Abst. 666) q Pre-Tx: Resistance testing was most likely ordered in patients: § with CD 4 cell count <350 cells/mm 3 (0 R 1. 64; 95%CI 1. 26 to 2. 15) § initiating Tx in the past 3 years (0 R 3. 65; 95%CI 2. 81 to 4. 73) q During HAART: Resistance testing was most likely ordered in: § females, IVD users, patients with high p. VL, patients with adherence <95% q Mortality: § No tested before Tx initiation 1. 7 -fold higher risk of mortality § Fewer resistance testing while on HAART 2. 7 -fold higher risk of mortality These results do not allow to establish a causal relationship regarding the association between physician-ordered genotypic resistance testing and survival.
Outcomes of HIV Drug Resistance
Outcomes of HIV Drug Resistance Residual Viremia (Abst. 664) < 50 HVI-1 RNA copies / m. L Clinical Implications ?
Transmission of Drug-resistant HIV
Transmission of Drug-resistant HIV Pre-Exposure Proxylaxis - Pr. EP (Abst. 678) q Pr. EP could substantially reduce HIV in San Francisco, but could also increase levels of Transmitted Drug Resistance § Based on “complex” mathematical models … § Assumptions: Pr. EP used by a median of 70% of MSM with a median efficacy of 60% in a population with a 10% transmitted drug resistance Preventing 58% of new infections next 10 years San Francisco Increasing TDR up to 31%
A final and global view. . .
WHO Updated List of Mutations for Surveillance of TDR HIV (Abst. 689) PI 23 I, 24 I, 0 N, 32 I, 46 I/L, 47 V/A, 48 M/V, 50 V/L, 53 L/Y, 54 V/M/L/T/S/A, 58 E, 73 S/T/C/A, 76 V, 82 A/F/L/T/S/M/C, 83 D, 84 V/A/C, 85 V, 88 D/S, 90 M NRTI 41 L, K 65 R/N, 67 N/G/E/del, 69 D/G/N/ins, 70 E/R/G, 74 I/V, 75 T/A/M/S, 77 L, 115 F, 116 Y, 151 M, 184 V/I, 210 W, 215 C/D/E/F/V/Y/S/I, 219 E/Q/ N/R NNRTI 100 I, 101 E, 103 N, V 106 A/M, 179 F, 181 C/I/V, 188 L/C, 190 A/S/E/Q/C, 225 H, 230 L, 236 L new mutations italicized • Examined expert lists: IAS–USA, Los Alamos, Stanford HIV Database, ANRS, and Rega • Analyzed numbers of subtype B and non-B sequences: 7395 and 7710 from PI-naive persons; and 5539 and 5982 from RTI-naïve persons. • Numbers of non-B sequences from untreated persons were: A, 1, 524; AE, 890; AG, 1, 415; C, 2, 145; D, 512; F, 605; G, 619. • Non-polymorphic mutations associated with ART were included in the list.