10 minutes for Ive got a bad back

10 minutes for “I’ve got a bad back” Kizzy, Vasu, Amer, Ramesh, Audrey, Ewan and Gill

Why it is important • LBP is not a homogenous condition • LBP is very common in working-age adults ( between the ages of 40 and 60 years ) • Treating all types of back pain costs the NHS more than £ 1000 million per year • In 1998 the direct healthcare costs of all back pain estimated at £ 1623 million -approximately 35% were related to private sector • The costs of care for LBP exceed £ 500 million/year • Lost production as a result of LBP costs at least £ 3500 million/year.

• LBP results in • • • impaired quality of life long-term morbidity a higher risk of social exclusion reduced income reliance on sickness benefits • Aims of interventions and therapies • manage disability and pain, • to help people to cope with day-to-day life, • to reduce distress, to enable people to remain in or return to work, • to minimise risk of recurrence.

History • • • Circumstances of pain Nature/severity of pain Associated symptoms PMH Exclude other sites of pain

Red Flags - age <20 or >55, – non mechanical pain, – worse when supine, – night time pain, – thoracic pain, – past hx of carcinoma, HIV, immunosuppression, IVDU, taking steroids, unwell, weight loss, – widespread neurology, structural deformity, saddle anaesthesia, incontinence bowel or bladder or retention of urine
")
Examination • • Deformity Palpate Movements Lower limbs (power, tone, sensation, reflexes, SLR)

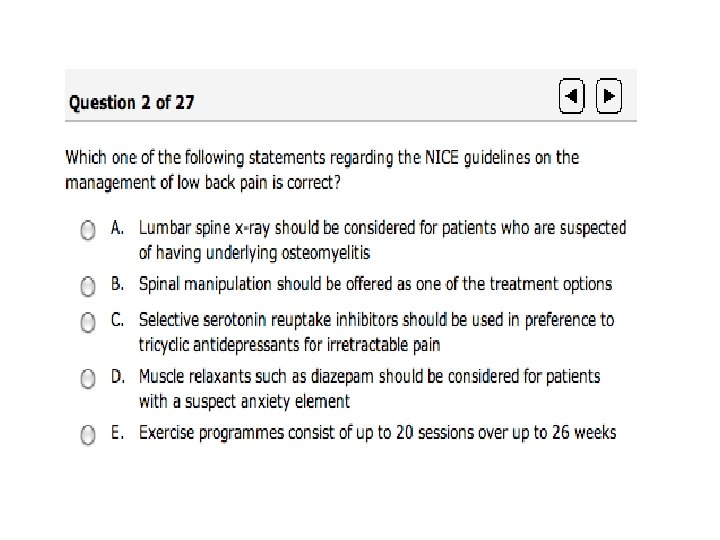
NICE guideline May 2009 Management of Low Back Pain Principles of management • Keep diagnosis under review at all times • Promote self-management: advise people with low back pain to exercise, be physically active and to carry on with normal activities as far as possible • Offer drug treatments as appropriate to manage pain and to help people keep active • Offer one of the following treatments, taking patient preference into account: – exercise programme – course of manual therapy – course of acupuncture

Advice and education • Provide advice and information to promote selfmanagement • Offer educational advice that: – includes information on the nature of non-specific low back pain – encourages normal activities as far as possible • Advise people to stay physically active and to exercise • Include an educational component • When considering recommended treatments, take into account the person’s expectations and preferences

Drug treatments • • • Option 1: Paracetamol: – Advise regular paracetamol as the first option Option 2: NSAIDS and / or weak opioids – Decision based on individual risk of side effects and patient preference – Give due consideration to risk of opioid dependence and side effects Option 3: Tricyclic antidepressants – Consider offering if other medications are insufficient, starting at a low dose and increase up to the maximum antidepressant dosage until • Therapeutic effect is achieved • Unacceptable side effects prevent further increases Option 4: Strong opioids (buprenorphine, fentanyl, oxycodone, high dose tramadol) – Consider offering for short-term use to people in severe pain – Consider referral if requires prolonged use – Consider risk of opioid dependence and side effects Co-prescribe a PPI for people over 45 For all medications, base decisions on continuation on individual response

Non-drug treatments • Structured exercise programme: – up to 8 sessions over up to 12 weeks – supervised group exercise programme in a group of up to 10 people, tailored to the person – one-to-one supervised exercise programme only if a group programme is not suitable • Manual therapy: – course of manual therapy, including spinal manipulation – up to 9 sessions over up to 12 weeks • Acupuncture: – course of acupuncture needling – up to 10 sessions over up to 12 weeks

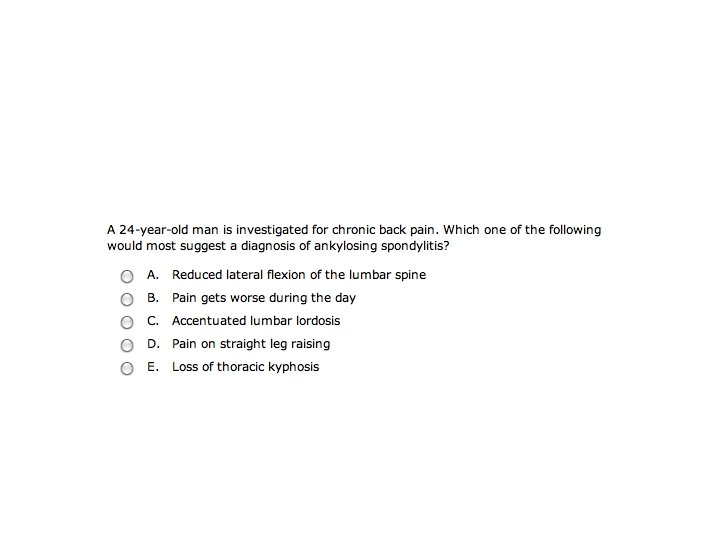
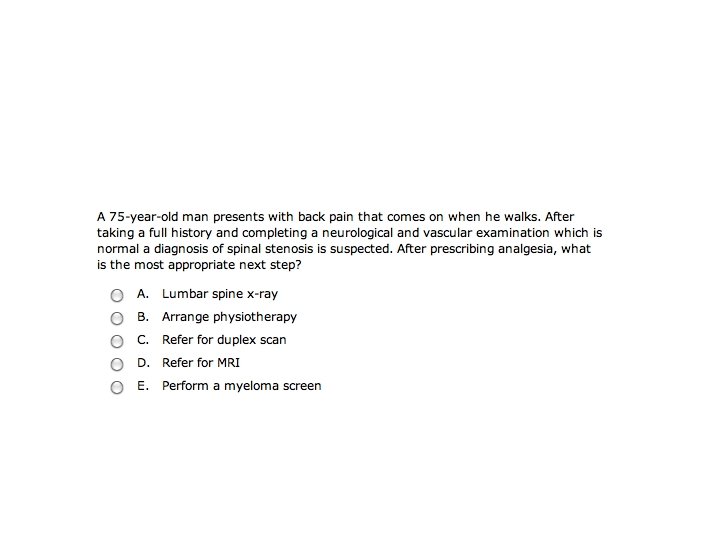
Imaging • Do not offer X-ray of the lumbar spine • Only offer MRI for non-specific low back pain in the context of a referral for an opinion • Consider MRI if one of these diagnoses is suspected: – spinal malignancy – cauda equina syndrome – Infection – Ankylosing spondylitis – Fracture – inflammatory disorder

Do Not offer…. • • SSRIs for treating pain Injections of therapeutic substances into the back Laser therapy Interferential therapy Therapeutic ultrasound TENS Lumbar supports Traction

AKT

Question 5 • An 18 yr old fast bowler presents with sudden onset of pain while extending his hip, and he walks with scoliosis. • A) scheurmanns disease • B) Spondylolisthesis • C) Acute disc prolapse • D) TB of spine

Question 6 • Following total hip replacement performed via posterior approach, the patient was noted to have a foot drop • A) Nuerapraxia of common peroneal nerve • B) Neurapraxia of Sciatic nerve • C) Neurapraxia of Calcaneal nerve • D) Neuropraxia of Femoral Nerve

Question 7 7. Which of the following are ‘red flags’ for possible serious spinal pathology? a)Age over 55 b)Anorexia c) Systemic steroid therapy d) Difficulty with micturition e) Cough-impulse pain • •

Question 8 8. How much radiation is involved in a plain lumbar spine X-ray compared to a chest Xray? a) Equal amounts b) Lumbar spine = 2 x Chest X-Ray c) Lumbar spine = 20 x Chest X-Ray d) Lumbar spine = 150 x Chest X-Ray

Question 9 9. What proportion of the population will develop low back pain at some time their lives? a) 20% b) 50% c) 70% d) 90%

Question 10 10. Low back pain is generally understood to become ‘chronic’ after a period of how long? a)6 weeks b)8 weeks c) 10 weeks d)12 weeks e)14 weeks

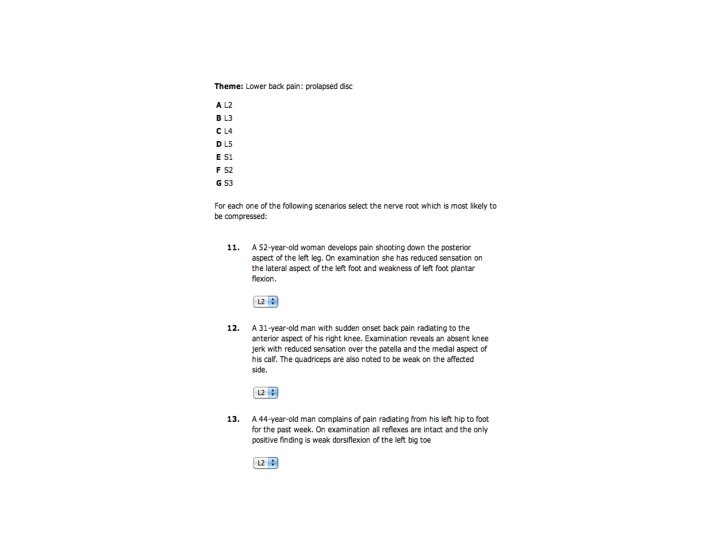
Answers • • • 1: B 2: A 3: S 1, L 4, L 5 4: D 5: C 6: B 7: A, C, D 8: D 9: C 10 : D

CSA scenario • Vasu has prepared a case for the day and will act as the patient.

Thankyou Any questions ?
- Slides: 26