1 Staging Classification and Treatment of Gestational Trophoblastic

1

Staging, Classification and Treatment of Gestational Trophoblastic Disease Assoc. Prof. Gazi YILDIRIM, M. D. Yeditepe University, Medical Faculty Dept of Ob&Gyn

Objectives • To define – Mol pregnancy – Malignant gestational trophoblastic tumors • To learn – Management of GTN

Classification • • Histological classification Partial mole Complete mole Invasive mole Metastatic mole Choriocarcinoma Placental-site trophoblastlc tumour Epithelioid trophoblastic tumour • • • Clinical classification of gestational trophoblastlc neoplasla Non-metastatic Metastatlc Low risk High risk
 Malignant • Invasive")
Types of GTD Benign • Hydatidiform mole/molar pregnancy (complete or incomplete) Malignant • Invasive mole • Choriocarcinoma (chorioepithelioma) • Placental site trophoblastic tumor

Hydatidiform mole
 • Histologically chorionic villi consist of trophoblastic proliferation and Edema")
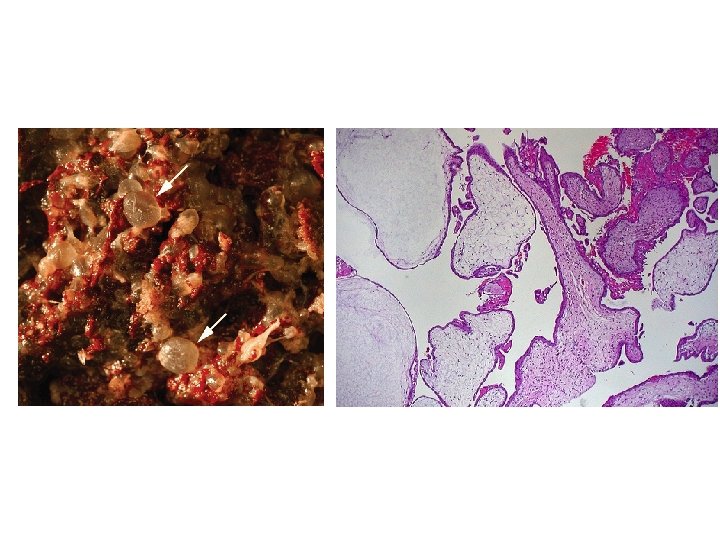
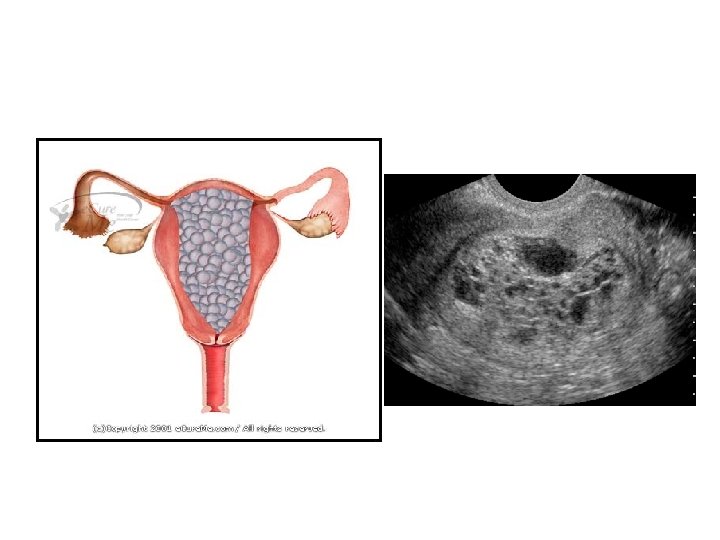
HYDATIDIFORM MOLE (MOLAR PREGNANCY) • Histologically chorionic villi consist of trophoblastic proliferation and Edema of villous stroma • Moles usually occupy the uterine cavity • The absence or presence of a fetus or embryonic elements has been used to describe them as complete and partial moles

COMPLETE HYDATIDIFORM MOLE • Chorionic villi transform into a mass of clear vesicles • Vesicles vary in size • The histological structure typically shows: 1. Hydropic degeneration and swelling of the villous stroma. 2. Absence of blood vessels in the swollen villi. 3. Proliferation of the trophoblastic epithelium to a varying degree 4. Absence of fetus and amnion.

• Chromosomal composition in 85 percent of complete molar pregnancies is 46, XX, with both chromosomes being of paternal origin • This phenomenon is termed androgenesis. • Typically, the ovum has been fertilized by a haploid sperm, which then duplicates its own chromosomes after meiosis. • The chromosomes of the ovum are either absent or inactivated. • Occasionally, the chromosomal pattern in a complete mole may be 46, XY due to dispermic fertilization
 Empty")
COMPLETE MOLE Empty ovum 46 XX 23 X Complete Mole (46 XX diploid) Empty ovum 23 X A single sperm fertilizes an empty ovum, with duplication of the 23 X haploid set of chromosomes, giving rise to a homozygous diploid complete mole. 46 XX or 46 XY 23 X or Y Two sperms with two independent haploid sets of chromosomes fertilize an empty ovum, producing a dyspermic complete mole with either 46 XX or 46 XY karyotype. Complete Mole (46 XX or 46 XY, diploid) Modified from Cheung, 1995


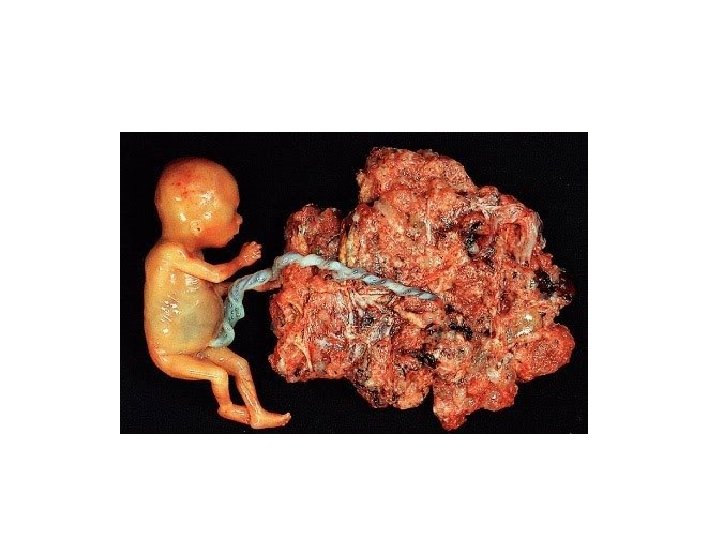
PARTIAL HYDATIDIFORM MOLE • Hydatidiform changes are focal and less advanced • Some element of fetal tissue is seen • There is slowly progressive swelling within the stroma of characteristically avascular chorionic villi • Other vascular villi with a functioning fetal-placental circulation • Karyotype typically is triploid 69, XXX, 69, XXY, or 69, XYY • These are each composed of one maternal and two paternal haploid sets of chromosomes • Nontriploid partial moles have been reported • The nonviable fetus of a triploid partial mole typically has multiple malformations • Abnormal growth is common • 82 percent of fetuses had symmetrical growth restriction.

PARTIAL MOLE 23 Y 23 X 23 X 69 XXY 23 Y Dyspermy 23 X/23 Y or 23 X/23 X Partial Mole (69 XXY, or 69 XXX, or 69 XYY triploid) Fertilization of a normal 23 X haploid ovum by two sperms, producing a triploid partial mole with either 69 XXY, 69 XXX or 69 XYY karyotype Modified from Cheung, 1995

• A twin gestation of a complete mole and a normal fetus and placenta is sometimes misdiagnosed as a diploid partial mole • Twin pregnancies consisting of a normal fetus and a complete mole have a substantively increased risk of developing gestational trophoblastic neoplasia • Generally, gestational trophoblastic neoplasia follows 20 percent of complete moles, whereas it develops in only 0. 5 percent of women after a partial mole • The risk of choriocarcinoma arising from a partial mole is also low
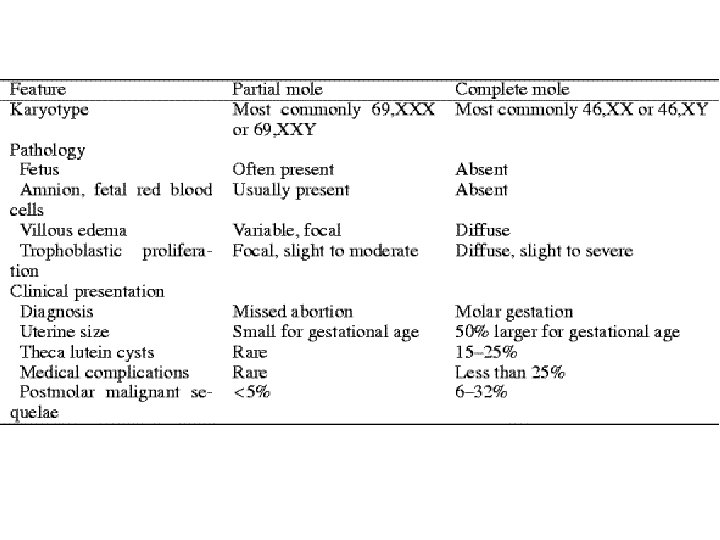

FEATURES OF PARTIAL AND COMPLETE MOLE Complete mole Partial mole Fetal or embryonic tissue absent present Hydatiform swelling of chorionic villi extensive focal Trophoblastic hyperplasia extensive focal Scalloping of chorionic villi absent present Trophoblastic stromal inclusions absent present Karyotype 46 XX (90%); Triploid (69 XXY) 46 XY (10%) Cohn DE, Herzog TJ. Curr Opin Oncol 2000 Sep; 12(5): 492 -6

INCIDENCE AND RISK FACTORS • Hydatidiform mole develops in approximately 1 in 1000 pregnancies in the United States and Europe. • Although it has been reported to be more frequent in other countries, especially in parts of Asia • The role of gravidity, estrogen status, oral contraceptives, and dietary factors in the risk of gestational trophoblastic disease is unclear

• Age. incidence of molar pregnancy highest in women aged 15 years or younger, and those aged 45 years or older. • In the latter group, the relative frequency of the lesion is at least 10 times greater than that at ages 20 to 40 years

• Previous Mole. Women with molar pregnancies are at increased risk of developing either a complete or a partial mole in a future pregnancy • Recurrent moles 1. 3 percent • Oocyte problem leads to molar development

CLINICAL COURSE. • Bleeding. • Vary from spotting to profuse hemorrhage. • There may be considerable hemorrhage concealed within the uterus. • Iron-deficiency anemia is common

• Uterine Size. • Growing uterus often enlarges more rapidly than usual • Exceeding in about half of cases that expected from the gestational age. • The uterus may be difficult to identify precisely by palpation because of its soft consistency. • Fetal Activity. • Typically no fetal heart motion is detected. • There may be incomplete molar degeneration in the placenta accompanied by a living fetus.

• Gestational Hypertension. • Because hypertension caused by pregnancy is rarely seen before 24 weeks, preeclampsia that • develops before this gestational age may be from hydatidiform mole or extensive molar degeneration. • Hyperemesis. • Significant nausea and vomiting may develop. • Thyrotoxicosis. • Plasma thyroxine levels in women with molar pregnancy are often elevated, but clinically apparent hyperthyroidism is unusual • Hyperthyroidism is identified in about 2 percent. • Serum free thyroxine is elevated as the consequence of the thyrotropin-like effect of h. CG

• Embolization. • Variable amounts of trophoblastic cells escape from the uterus into the venous outflow at the time of molar evacuation • The volume may be such as to produce signs and symptoms of acute pulmonary embolism or edema. • This tissue can subsequently invade the pulmonary parenchyma to establish metastases.

DIAGNOSTIC FEATURES • To summarize, the clinical and diagnostic features of a complete hydatidiform mole are: 1. Continuous or intermittent brown or bloody discharge evident by about 12 weeks and usually not profuse. 2. Uterine enlargement out of proportion to the duration of pregnancy in about half of the cases. 3. Absence of fetal parts and fetal heart motion. 4. Characteristic ultrasonographic appearance. 5. Serum h. CG level higher than expected for the stage of gestation. 6. Preeclampsia-eclampsia developing before 24 weeks. 7. Hyperemesis gravidarum.

PROGNOSIS • Mortality from molar pregnancies has been practically reduced to zero by prompt diagnosis and appropriate therapy. • Earlier evacuation has not reduced the 20 percent risk for gestational trophoblastic neoplasia

TREATMENT • Hydatidiform mole treatment consists of two phases. The first is immediate evacuation of the mole, The second is subsequent evaluation for persistent trophoblastic proliferation or malignant change. – Computed tomography or magnetic resonance imaging to evaluate the liver or brain is not performed routinely.

• Prophylactic Chemotherapy. • Controversial • Toxicity from prophylactic chemotherapy may be significant • Chemoprophylaxis may be considered in women with high-risk complete moles, particularly if serum h. CG testing is unavailable or follow-up is impossible

• • Vacuum Aspiration. Treatment of choice for hydatidiform mole Cervical dilating agents may be necessary The cervix may be further dilated under anesthesia to a diameter sufficient to allow insertion of a suction curet. • After most of the molar tissue has been removed by aspiration, oxytocin is given. • Intraoperative ultrasonographic examination may help document that the uterine cavity has been emptied.

• Oxytocin, Prostaglandins, and Hysterotomy. • Labor induction rarely is used for evacuation of hydatidiform moles. • Hysterectomy. • If no further pregnancies are desired, hysterectomy may be preferred to suction curettage. • Hysterectomy does not eliminate recurrent disease, it appreciably reduces likelihood

FOLLOW-UP EVALUATION OF MOLAR PREGNANCY 1. Prevent pregnancy for a minimum of 6 months using hormonal contraception. 2. Monitor serum h. CG levels every 2 weeks. Serial measurement of serum h. CG is important to detect trophoblastic neoplasia, 3. Chemotherapy is not indicated as long as these serum levels continue to regress. A rise or persistent plateau in the level demands evaluation for gestational trophoblastic neoplasia An increase signifies trophoblastic proliferation that is most likely malignant unless the woman is again pregnant. 4. Once the h. CG level falls to a normal level, test the patient monthly for 6 months; then follow-up is discontinued and pregnancy allowed. • Estrogen-progestin contraceptives or depot-medroxyprogesterone usually are used to prevent a subsequent pregnancy during the period of surveillance.

GESTATIONAL TROPHOBLASTIC NEOPLASIA • Also called malignant gestational trophoblastic disease, • Refers to – invasive mole, – choriocarcinoma, – placental site trophoblastic tumor. • Any of these may follow molar pregnancy or normal pregnancy, or develop after abortive outcomes, including ectopic pregnancy.

ETIOLOGY • Gestational trophoblastic neoplasia almost always develops with or follows some form of pregnancy. • Approximately – 50% of cases follow a hydatidiform mole, – 25% follow an abortion, – 25% percent develop after an apparently normal pregnancy.

PATHOLOGY • The diagnosis of gestational trophoblastic neoplasia is made primarily by persistently elevated serum h. CG levels.

Choriocarcinoma

Definition A malignant form of GTD which can develop from a hydatidiform mole or from placental trophoblast cells associated with a healthy fetus , an abortion or an ectopic pregnancy.

Definition • Characterized by abnormal trophoblastic hyperplasia and anaplasia , absence of chorionic villi

Gross specimen of choriocarcinoma

Microscopic image of choriocarcinoma absence of chorionic villi

Common Sites for Metastatic Gestational Trophoblastic Tumors Site Lung Vagina Vulva/cervix Brain Liver Kidney Spleen Gastrointestinal Per cent 60 -95 40 -50 10 -15 5 -15 0 -5 0 -5

Invasive mole

Definition This term is applied to a molar pregnancy in which molar villi grow into the myometrium or its blood vessels, and may extend into the broad ligament and metastasize to the lungs, the vagina or the vulva.

Invasive mole: the tissue invades into the myometrial layer. No obvious borderline, with obvious bleeding.

Invasive hydatidiform mole infiltrating the myometrium
")
Placenta Site Trophoblastic Tumor (PSTT)

Definition • Placenta Site Trophoblastic Tumor is an extremely rare tumor that arised from the placental implantation site • Tumor cells infiltrate the myometrium and grow between smooth-muscle cells


• Placental Site Trophoblastic Tumor. • Trophoblastic neoplasia arises from the placental implantation site following a normal term pregnancy, spontaneous or induced abortion, ectopic pregnancy, or molar pregnancy • Histologically predominantly cytotrophoblastic cells, and immunohistochemical staining reveals many prolactinproducing cells and few gonadotropin-producing ones • Thus, serum h. CG levels may be normal to elevated. • Bleeding is the main presenting symptom. • h. PL is high (human Placental Lactogen)

Dignosis and treatment of GTN • Surum h. CG levels are relatively low compared to those seen with choriocarcinoma. • Several reports have noted a benign behavior of this disease. They are relatively chemotherapyresistant, and deaths from metastasis have occurred. • Surgery has been the mainstay of treatment

CLINICAL COURSE • The most common finding is irregular bleeding associated with uterine subinvolution. • The bleeding may be continuous or intermittent, with sudden and sometimes massive hemorrhage. • Uterine perforation caused by invasive trophoblastic growth may cause intraperitoneal hemorrhage • Metastatic lesion of the vagina or vulva • Untreated, choriocarcinoma is invariably fatal.

Symptoms and signs • • • Bleeding Infection Abdominal swelling Vaginal mass Lung symptoms Symptoms from other metastases
 ≤ 39")
WHO Prognostic Scoring System Score Prognostic factor 0 1 2 4 Age(years) ≤ 39 >39 — — Pregnancy history Hydatidiform Abortion, mole ectopic Term pregnancy — Interval (months) of treatment <4 4 -6 7 -12 >12 Initial h. CG(m. IU/ml) <103 103 -104 104 -105 >105 Largest tumor(cm) <3 3 -5 >5 — Sites of metastasis Lung Spleen, kidney GI tract, liver Brain No. of metastasis — 1 -4 4 -8 8 Previous (treatment) — — Single drug 2 or more 0 -4 low risk, 5 -7 intermediate risk, >8 high risk for death

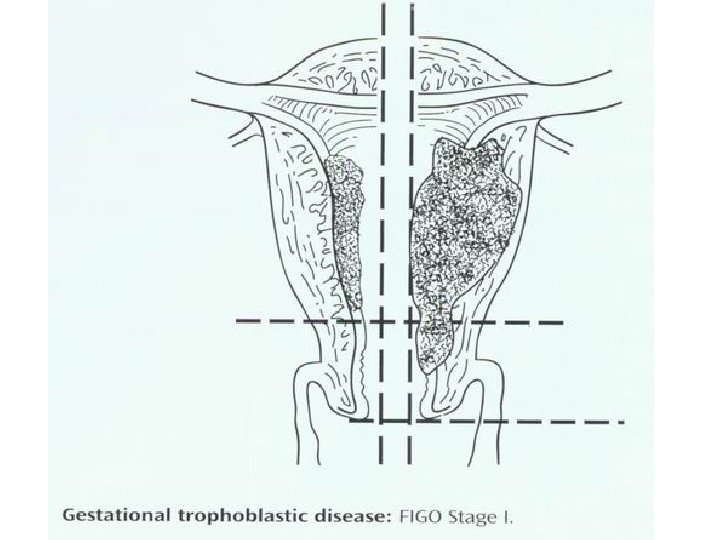
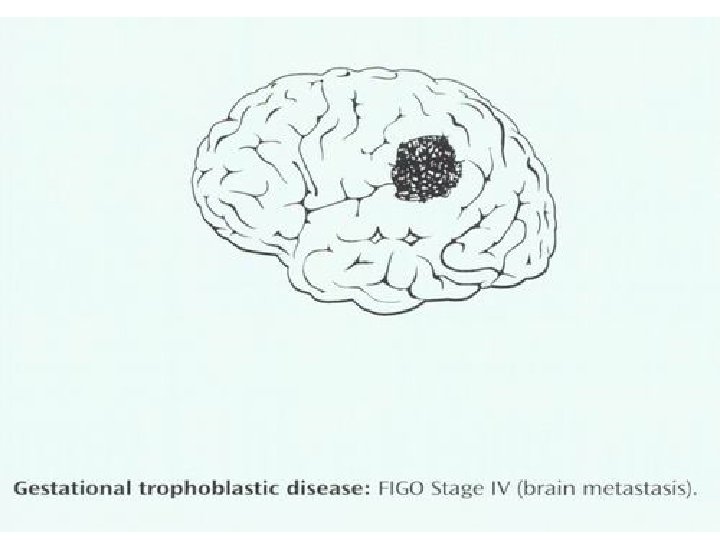
FIGO Staging System for Gestational Trophoblastic Tumors Stage Ⅰ Ⅱ Ⅲ Ⅳ Description Limited to uterine corpus Extends to the adnexae, outside the uterus, but limited to the genital structures Extends to the lungs with or without genital tract All other metastatic sites

FIGO Staging System for Gestational Trophoblastic Tumors • Substages assigned for each stage as follows: A: No risk factors present B: One risk factor C: Both risk factors • Risk factors used to assign substages: 1. Pretherapy serum h. CG > 100, 000 ml. U/ml 2. Duration of disease >6 months

IIa IIb

IIIa<3 cm or locate in half lung IIIb disease beyond IIIa

Diagnosis and evaluation • Gestational trophoblastic tumor is diagnosed by rising h. CG following evacuation of a molar pregnancy or any pregnancy event • Once the diagnosis established the further examinations should be done to determine the extent of disease ( X-ray, CT, MRI)

Treatment • Nonmetastatic GTD • Low-Risk Metastatic GTD • High-Risk Metastatic GTD

Treatment of Nonmetastatic GTD • Hysterectomy is advisable as initial treatment in patients with nonmetastatic GTD who no longer wish to preserve fertility • This choice can reduce the number of course and shorter duration of chemotherapy. • Adjusted single-agent chemotherapy at the time of operation is indicated to eradicate any occult metastases and reduce tumor dissemination.

Treatment of Nonmetastatic GTD • Single-agent chemotherapy is the treatment of choice for patients wishing to preserve their fertility. • Methotrexate(MTX) and Actinomycin-D are generally chemotherapy agents • Treatment is continued until three consecutive normal h. CG levels have been obtained and two courses have been given after the first normal h. CG level. To prevent relapse or metastasis

Treatment of Low-Risk Metastatic GTD • Single-agent chemotherapy with MTX or actinomycin. D is the treatment for patients in this category • If resistance to sequential single-agent chemotherapy develops, combination chemotherapy would be taken • Approximately 10 -15% of patients treated with singleagent chemotherapy will require combination chemotherapy with or without surgery to achieve remission

Treatment of High-Risk Metastatic GTD • Multiagent chemotherapy with or without adjuvant radiotherapy or surgery should be the initial treatment for patients with high-rist metastatic GTD • EMA-CO regimen formula is good choice for high-rist metastatic GTD • Adjusted surgeries such as removing foci of chemotherapy-resistant disease, controlling hemorrhage may be the one of treatment regimen

EMA-CO Chemotherapy for poor Prognostic Disease 100 mg/M 2 IV daily× 2 days (over 30 -45 minutes) Methotrexate 100 mg/M 2 IV losding dose, then 200 mg/M 2 over 12 hours day 1 Actinomycin D 0. 5 mg IV daily× 2 days Folinic acid 15 mg IM or p. o. q 12 hours× 4 starting 24 hours after starting methotrexate Cyclophosphamide 600 mg/M 2 Etoposide(VP-16) Oncovin (vincristine) 1 mg/M 2 (Repeat every 15 days as toxicity permits) IV on day 8

Prognosis • Cure rates should approach 100% in nonmetastatic and low-risk metastatic GTD • Intensive multimodality therapy has resulted in cure rates of 80 -90% in patients with high-risk metastatic GTD

Follow-up After Successful Treatment • Quantitative serum h. CG levels should be obtained monthly for 6 months, every two months for remainder of the first year, every 3 months during the second year • Contraception should be maintained for at least 1 year after the completion of chemotherapy. Condom is the choice.

• Placental Site Tumors. • Hysterectomy is the most efficacious treatment for confirmed placental site trophoblastic tumor • It is not necessary to remove the ovaries if they appear normal • Although chemotherapy is recommended for metastatic disease, it is not as effective as for other gestational trophoblastic neoplasias

PREGNANCY AFTER GESTATIONAL TROPHOBLASTIC DISEASE • • Follow-up surveillance is minimally 6 months for molar pregnancy 1 year for gestational trophoblastic neoplasia Up to 2 years for cases with metastases other than to the lung. There is no difficulty with fertility or normal pregnancy outcome following • Successfully treated gestational trophoblastic disease • Women who have been given chemotherapy do not have an increased risk for anomalous fetuses in subsequent pregnancies • The primary concern is that women who had gestational trophoblastic disease are at increased risk for developing it again in a subsequent pregnancy.
- Slides: 71