1 Natural History of Type 2 Diabetes Progression

1

Natural History of Type 2 Diabetes Progression Years from-10 diagnosis -5 0 5 10 15 Insulin resistance Insulin secretion Microvascular complications Macrovascular Pre-diabetes complications Type 2 diabetes (T 2 DM) Onset Diagnosis 2

Risk of Microvascular Complications vs. A 1 C in Type 1 Diabetes Results From the DCCT Relativ 20 e risk Retinopathy progression Neuropathy progression Microalbuminuria progression 15 10 5 0 1 5 6 7 8 9 10 11 12 A 1 C (%) Skyler JS. Endocrinol Metab Clin North Am. 1996; 25: 243 -254 4

Lessons from UKPDS: Better control in T 2 DM means fewer complications 1% reduction in Hb. A 1 c Risk reduction* Deaths from diabetes -21% Myocardial Infarction -14% Microvascular complications -37% 1% Peripheral vascular disorders *p<0. 0001 n=3, 642 type 2 diabetes patients 1. Stratton IM et al. BMJ 2000; 321: 405– 412 -43%

The benefits of early tight control: UKPDS 10 -year post-trial follow-up

Early Insulinization Prevents the Progressive β-cell Dysfunction Early intensive insulin therapy has favorable Insulin provides a type outcomes on recovery of β-cell rest and maintenance of reduce excessive β-cell function secretory demands compared with oral hypoglycemic agents Weng JP et al. Lancet, 2008, 301: 1753 -1780 on damaged β-cell

Hb. A 1 c targets in current guidelines ADA/EASD IDF NICE AACE France Canada Australia Latin America Hb. A 1 c target (%) <7 <7 <6. 5 ≤ 6. 5 <6. 5 ≤ 7 <6. 5

Only around one-third of patients* in developing countries achieve Hb. A 1 c <7% Patients* with Hb. A 1 c <7% (%) The International Diabetes Management Practice Study (IDMPS) *Patients with Hb. A 1 c test (36% of overall population) Chan JC, et al. Diabetes Care 2009; 32: 227– 33.
* Fewer than 5% of patients in developing countries achieve glycaemic")
Patients achieving goals (%)* Fewer than 5% of patients in developing countries achieve glycaemic and CV goals The International Diabetes Management Practice Study (IDMPS) *Hb. A 1 c <7%, blood pressure 130/80 mm. Hg, LDL-C <100 mg/d. L Chan JC, et al. Diabetes Care 2009; 32: 227– 33.

Clinical inertia: ‘Failure to advance therapy when recommended’ Mean Hb. A 1 c at last visit (%) 10 9 8 ADA goal 7 9. 6% 8. 6% Diet & exercise 2. 5 years 8. 9% Combination oral agents SU or metformin 2. 9 years 2. 8 years Years since initial diagnosis 8. 2 years Initiation of insulin therapy Brown JB, et al. Diabetes Care 2004; 27: 1535– 40.

Delaying insulinisation results in increased A 1 C Mean A 1 C at last visit (%) 10 Sulfonylurea or metformin monotherapy Combination therapy Insulin Diet/exercise 9 8 ADA/ EASD goal 7 <7% 6 0 2 Diagnosis Brown JB, et al. Diabetes Care 2004; 27: 1535− 40 3 4 5 Years 6 7 8 9 10

Stepwise management of T 2 DM Biggest clinical hurdle? ? ? Ins co Or bi al na tio n Or al ins plu uli s n m mo Di ex et & er cis e O no ral th er ap uli n + + + y Adapted from Williams G. Lancet 13 1994; 343: 95– 100.
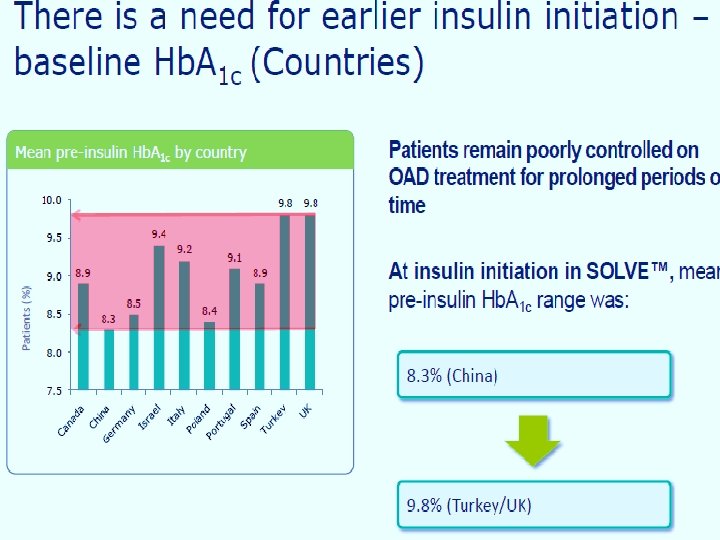
 ACHIEVE study: Insulin therapy started")
Multinational, observational study of T 2 DM (66, 726) ACHIEVE study: Insulin therapy started in routine clinical care when Hb. A 1 c 9. 3– 9. 8%: China S. Asia E. Asia N. Africa Mid East Lat. Am. Russia n 9, 493 21, 107 9, 062 3, 623 11, 971 1, 032 2, 954 Age (yrs) 55. 7 51. 7 56. 5 58. 3 52. 8 59. 6 59. 2 T 2 DM (yrs) 7. 9 6. 7 12. 5 11. 4 10. 2 15. 5 9. 6 Complications (%) 86. 1 94. 0 90. 3 89. 7 79. 9 90. 7 96. 1 CV disease (%) 22. 9 32. 5 29. 4 28. 5 30. 5 35. 3 74. 6 Renal disease (%) 26. 1 28. 7 34. 6 36. 5 43. 6 41. 8 41. 7 Eye problems (%) 25. 6 22. 0 29. 9 41. 2 36. 8 41. 2 71. 0 Foot ulcer (%) 2. 5 6. 5 5. 8 3. 5 8. 7 7. 7 5. 1 Neuropathy (%) 33. 7 29. 4 40. 1 38. 9 56. 0 47. 6 84. 4 Adjusted for age at diagnosis; Complications (%) predicted from a logistic model Zilov AV, et al. Diabetes 2011; 60(Suppl. 1): 2485. Complications already present in people with T 2 DM when initiating insulin therapy
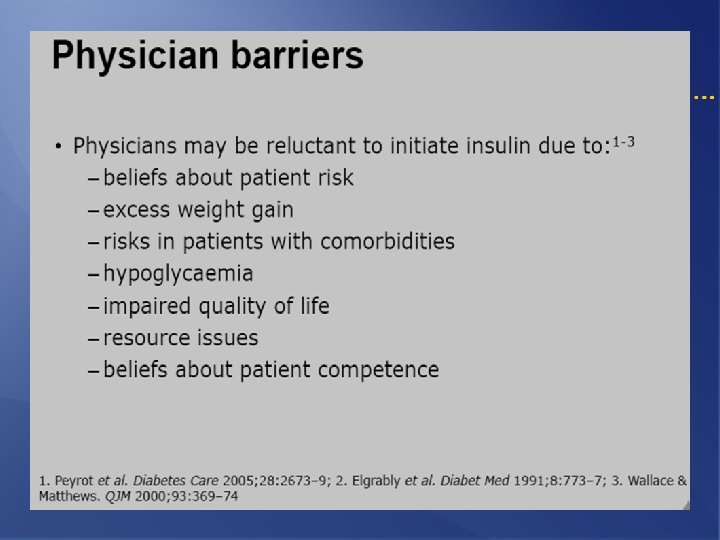

Clinical inertia: patient and physician barriers Peyrot et al. Diabetes Care 2005; 28: 2673– 9; Elgrably et al. Diabet Med 1991; 8: 773– 7; Wallace & Matthews. QJM 2000; 93: 369– 74; Kunt & Snoek. Int J Clin Pract 2009; 63(Suppl. 164): 6– 10
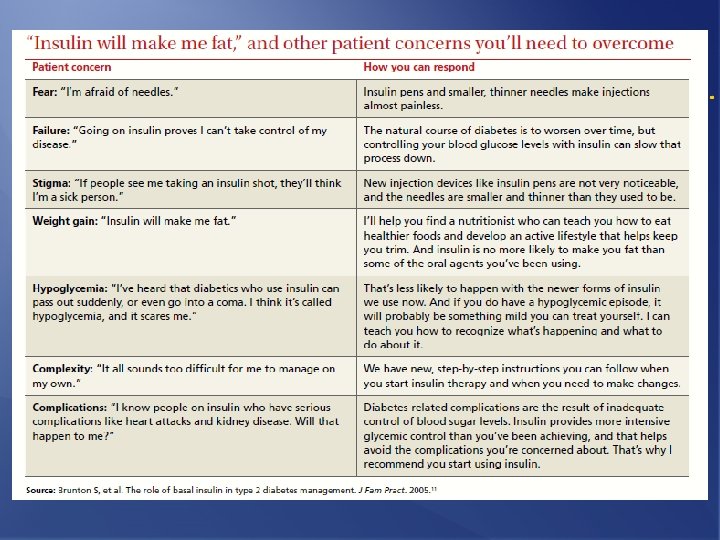

Barriers to insulin initiation Nakar et al. J Diabetes Complications 2007; 21: 220– 6

Vijan et al. J Gen Intern Med 2005; 20: 479– 82.
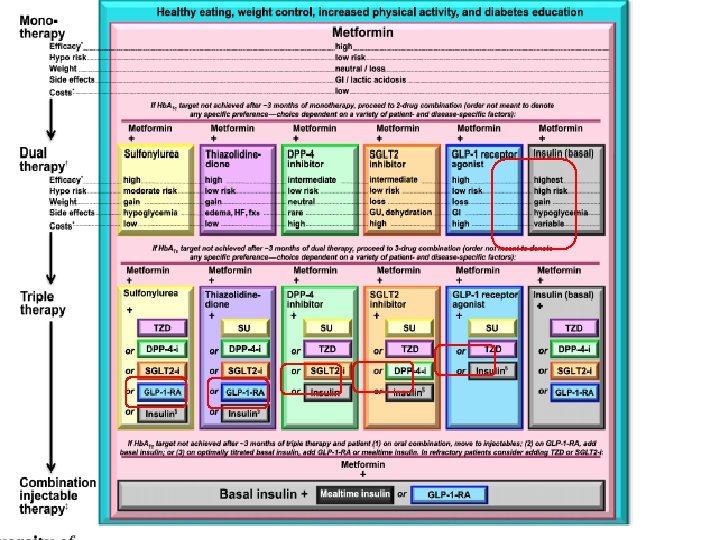

Figure 3. Approach to starting & adjusting insulin in T 2 DM Diabetes Care 2015; 38: 140; Diabetologia 2015; 10. 1077/s 00125 -014 -3460 -

Do not forget! beneficial effects of early insulin therapy in T 2 DM on morbidity and mortality, and l The total mortality. on ADA-EASD guideline, Basal Insulin, is the most convenient method for insulin initiation. l Based

So, why not to do! Start Insulin At The Right Time! Adjust & Follow!
- Slides: 24