1 DIABETES MELLITUS Kaveh Eslami Pharm D board

1

DIABETES MELLITUS Kaveh Eslami Pharm. D board certified Clinical pharmacist Tehran university of medical science ﺑﻮﺷﻬﺮ 1390 ﺑﻬﺸﺖ ﺍﺭﺩی 2
 2) 3) 4) ﺍﻧﻮﺍﻉ ﺩیﺎﺑﺖ Diabetes insipidus (DI)")
Diabetes ﻣﻌﻨﺎی ﻟﻐﺘی I. II. 1) 2) 3) 4) ﺍﻧﻮﺍﻉ ﺩیﺎﺑﺖ Diabetes insipidus (DI) Diabetes mellitus (DM) � � Type 1 (IDDM) Type 2 (NIDDM) Gestational DM Other specific type 3
 5")
DIABETES MELLITUS (DM) 5

8

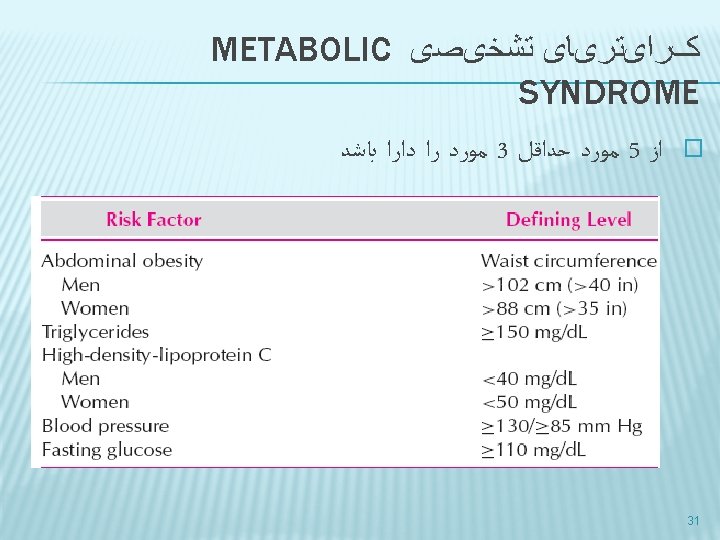
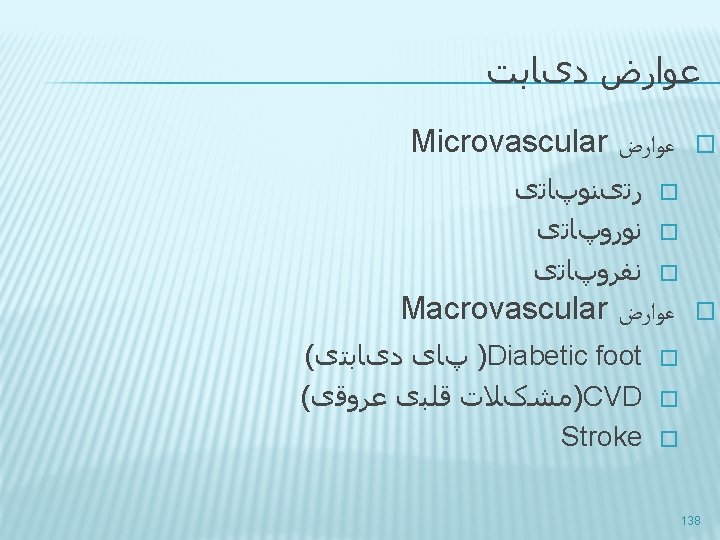
ﺩیﺎﺑﺖ ﻋﻮﺍﺭﺽ : ﺍﻫﻤیﺖ Macrovascular ﻭ Macrovascular ﻋﻮﺍﺭﺽ � � Morbidity & Mortality � Type 1: 5 -12 times � Type 2: 2 times � 2. 4 times more costly 9

HUMAN PROINSULIN AND ITS CONVERSION TO INSULIN 12

INSULIN � Made up of two polypeptide chains: α-21 AA; β 30 AA � Proinsulin, the precursor of insulin, single chain 86 AA � proinsulin→ Insulin+ C-peptide � Measurable C-peptide levels: endogenously produced insulin and functioning β-cell 13

14

15

EFFECTS OF INSULIN ON CARBOHYDRATE, FAT AND PROTEIN METABOLISM IN LIVER, MUSCLE AND ADIPOSE TISSUE 16

EFFECT ON BLOOD GLUCOSE � � Insulin has essential metabolic actions as a fuel-storage hormone and also affects cell growth and differentiation. It decreases blood glucose by: 1. 2. 3. 4. increasing glucose uptake into muscle and fat via Glut-4 increasing glycogen synthesis decreasing gluconeogenesis decreasing glycogen breakdown 17

DM; SYMPTOMS 20
 21")
TYPE 1 (IDDM) 21
 �")
DIABETES TYPE 1 � Earliest abnormality: first phase plasma insulin response (postprandial hyperglycemia) � Fasting hyperglycemia: 80 -90% reduced β cell mass 23

24

25

TREATMENT �Diet �Drugs: Insulin, oral hypoglycemic or antihyperglycemic �Exercise 29

Characteristics Percentage Age at onset Pancreatic func. Pathogenesis Type 1 Type 2 5 -10% 90% usually<30 yrs usually>40 yrs Usually none Low, NRL or high Insulin HLA types, ICA Defect in Ins secretion, tissue resistance, ↑hepatic glucose output Family history Obesity usually not strong Strong Uncommon Common(60 -90%) Ketoacidosis Often Rare Clinical presentation Treatment Moderate to severe Accidentally diagnosed Insulin Life saving Oral drug 32

ﺩیﺎﺑﺖ کﻨﻨﺪﻩ ﺍیﺠﺎﺩ ﺩﺍﺭﻭﻫﺎی � Nicotinic acid � Glucocorticoids � Thyroid hormone � Diazoxide � β-Adrenergic agonists � Thiazides � Phenytoin � α-Interferon 35
 FBS or FPG (")
ﺧﻮﻥ ﻗﻨﺪ گیﺮی ﺍﻧﺪﺍﺯﻩ ﺗﺴﺘﻬﺎی ( fasting blood sugar) FBS or FPG ( post prandial suga) PPS ﻗﻨﺪ ﺍﺩﺭﺍﺭ ( self monitoring blood glucose )SMBG Hb. A 1 c OGTT � � � 37

BLOOD GLUCOSE � Min plasma glucose Conc: 40 -60 mg/dl � CNS is independent of Ins � Muscle & Fat require Ins � Heart? 38

HGB A 1 C � 1% change in A 1 c ~ 35 mg/d. L change in mean plasma glucose concentration � A 1 c 7% ~mean plasma glucose 170 mg/d. L 42

46

Normal Fasting 0. 5, 1, 1. 5 hr 2 hr <100 <200 <140 140 -200 Impaired glucose tolerance Impaired fasting glucose Diabetes (nonpregnant) 100 -125 ≥ 126 ≥ 200 49
 � FBS 140 -200 100 -126 50")
PREDIABETES � PPS (2 h) � FBS 140 -200 100 -126 50

CATEGORIES OF INCREASED RISK FOR DIABETES 1. 2. 3. FPG 100 mg/dl to 125 mg/dl (IFG) OR 2 -h PG in the 75 -g OGTT 140 mg/dl to 199 mg/dl (IGT) OR A 1 C 5. 7– 6. 4% 51

ﻫﺪﻑ ﺍﺯ ﺩﺭﻣﺎﻥ 1. 2. 3. 4. control hyperglycemia reducing or preventing complications improving life expectancy improving quality of life 53

ADA GOALS FOR DIABETIC ADULTS � A 1 c � Preprandial BS � Postprandial BS � Blood pressure � LDL � TG � HDL Men women <7% 80 -120 mg/dl <160 mg/dl <130/80 mm. Hg <100 mg/dl <150 mg/dl >40 mg/dl >50 mg/dl 55

57


PREMIXED � NPH/Reg 70: 30 � Aspart protamin/ Aspart 70: 30 63

64

65

NOVOLOG® MIX 70/30 66

NOVOMIX 70% insulin aspart protamine suspension and 30% insulin aspart injection � one unit of Novo. Log has the same glucose-lowering effect as one unit of regular human insulin. � However, the effect of Novo. Log Mix 70/30 is more rapid in onset compared to Novolin ® (human insulin) 70/30 due to its faster absorption after subcutaneous injection. � 67

68

 is the preferred treatment for the conscious individual with")
HYPOGLYCEMIA Glucose (15– 20 g) is the preferred treatment for the conscious individual with hypoglycemia, although any form of carbohydrate that contains glucose may be used. � If SMBG 15 min after treatment shows continued hypoglycemia, the treatment should be repeated. � Once SMBG glucose returns to normal, the individual should consume a meal or snack to prevent recurrence of hypoglycemia. � 77
 given orally is the recommended treatment")
� � � Glucose (10 to 15 g) given orally is the recommended treatment in conscious patients. Dextrose IV may be required in individuals who have lost consciousness. Glucagon 1 mg intramuscular, is the treatment of choice in unconscious patients when IV access cannot be established only in type 1 78

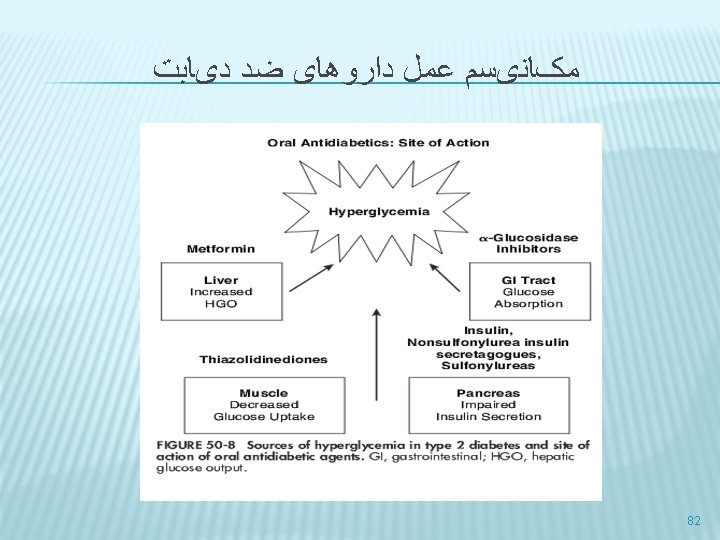
ﺩﺍﺭﻭﻫﺎی ﺿﺪ ﺩیﺎﺑﺖ 1. sensitizers � � 2. Insulin augmenting agent � � 3. Biguanides ( metformin) Thiazolidinediones ( Pioglitazone ) Short-acting ( nonsulfonylurea) insulin secretagogues ( repaglinide) Sulfonylurea ( glibenglamide ) Delayers of carbohydrate absorbtion � α- Glucosidase inhibitor ( Acarbose ) 81

ALGORITHM FOR THE METABOLIC MANAGEMENT OF TYPE 2 DIABETES 83

ALGORITHM FOR THE METABOLIC MANAGEMENT OF TYPE 2 DIABETES 84

ﺗﺮﺗیﺐ ﺍﺛﺮ ﺩﺍﺭﻭﻫﺎی ﺧﻮﺭﺍکی Biguanides Acarbose < Thiazolidinediones < Sulfonylurea repaglinide 85
 86")
BIGUANIDES METFORMIN (GLUCOPHAGE®) 86

BIGUANIDES DOSE � ﺩﻭﺯ ﺍﺑﺘﺪﺍیی ﺷﺒﻬﺎ ﺗﺠﻮیﺰ ﺷﻮﺩ ﻫﺮ ﺷﺐ ﻫﻤﺮﺍﻩ ﺑﺎ ﻏﺬﺍ 500 � ﺩﻭﺯ ﺍﺑﺘﺪﺍیی ﻫﻔﺘﻪ ﺍﻓﺰﺍیﺶ یﺎﺑﺪ 2 � ﺩﻭﺯ ﻫﺮ یک ﺗﺎ � We begin with 500 mg once daily with the evening meal and, if tolerated, add a second 500 mg dose with breakfast. � The dose can be increased slowly (one tablet every one to two weeks) as necessary � The usual effective dose is 1500 to 2000 mg/day per day; the maximum dose of 2550 mg/day (850 mg TID) provides only marginally better glycemic control and is often not tolerated due to GI side effects 92

Sulfonylurea 94

SULFONYLUREA 96

MECHANISM OF ACTION � � � The sulfonylurea receptor is a component of the potassium channel in the pancreatic ß-cells sulfonylurea binding leads to inhibition of these channels, which alters the resting potential of the cell, leading to calcium influx and stimulation of insulin secretion The net effect is increased responsiveness of ß-cells to both glucose and non-glucose secretagogues (such as amino acids), resulting in more insulin being released at all blood glucose concentrations Thus, sulfonylureas are useful only in patients with some ßcell function. Sulfonylureas may also have extrapancreatic effects, one of which is to increase tissue sensitivity to insulin, but the clinical importance of these effects is minimal 97
 � abnormal liver")
ﻋﻮﺍﺭﺽ � Hypoglycemia � nausea � skin reactions (including photosensitivity) � abnormal liver function tests � Weight gain 99

HYPOGLYCEMIA � Hypoglycemia is the most common side effect and is more common with long-acting sulfonylureas (such as chlorpropamide and glyburide) � The incidence was highest in those patients taking glyburide, and lowest among those taking tolbutamide 100

GLICLAZIDE DIAMICRON® Gliclazide has a duration of action of 12 to 24 hours � Because its effects are less prolonged than those of chlorpropamide or glibenclamide it may be more suitable for elderly patients, who are prone to hypoglycaemia with longer-acting sulfonylureas. � usual initial dose is 40 to 80 mg daily, gradually increased, if necessary, up to 320 mg daily � Doses of more than 160 mg daily are given in 2 divided doses � 103

REPAGLINDE NOVONORM � Tab 0. 5, 1, 2, 4 104
 108")
THIAZOLIDINEDIONES PIOGLITAZONE ( ACTOS®) 108
,")
MECHANISM � They bind to and activate one or more peroxisome proliferator-activated receptors (PPARs), which regulate gene expression in response to ligand binding � It appears that the thiazolidinediones improve insulin responsiveness in skeletal muscle by facilitating glucose transport activity � They thereby increasing rates of muscle glycogen synthesis and glucose oxidation. 109

EFFICACY � Thiazolidinediones are probably similar in efficacy to metformin as monotherapy. � we do not generally choose thiazolidinediones over metformin for initial therapy of type 2 diabetes due to concerns about adverse effects and cost 110

ADR Weight gain � Fluid retention/heart failure � decrease bone density and increase fracture risk in women � Hepatotoxicity � Macular edema � Eczema ( Rosiglitazone ) � LDL ( Rosiglitazone ) � CHF � Anemia � 111

HEPATIC AND RENAL IMPAIRMENT — No adjustment is necessary. � Therapy should not be initiated if the patient exhibits active liver disease or increased transaminases (>2. 5 times ULN) at baseline � During treatment if ALT levels elevate >3 times ULN, the test should be repeated as soon as possible. � If ALT levels remain >3 times ULN or if the patient is jaundiced, therapy should be discontinued. � 112

DRUG INTERACTIONS � Gemfibrozil � Induces CYP 3 A 4 113
 116")
Α- GLUCOSIDASE INHIBITOR ACARBOSE (GLUCOBAY®) 116

Insulin in type 2 DM 118

INSULIN THERAPY IN TYPE 2 DIABETES MELLITUS � once per day insulin should be added to oral hypoglycemic therapy in patients with type 2 diabetes � insulin NPH given at bedtime or insulin glargine given in the morning or at bedtime is a reasonable initial regimen � When switching to insulin monotherapy, it is reasonable to begin with a similar regimen consisting of basal insulin (NPH, detemir, or glargine insulin) given once or twice daily 119

INSULIN AS INITIAL THERAPY � Insulin can be considered initial therapy for all patients with type 2 diabetes, particularly patients presenting with � A 1 C >10 percent � fasting plasma glucose >250 mg/d. L � random glucose consistently >300 mg/d. L � ketonuria 120

PRE-MIXED AND SHORT ACTING INSULIN � Although we do not recommend pre-mixed insulin for the treatment of type 1 diabetes, it is a reasonable option for patients with type 2 diabetes who are doing well on a stable, fixed ratio � More complex insulin regimens can be used in patients with type 2 diabetes, in an attempt to achieve near normoglycemia by adding short- or rapid-acting insulin before meals. 121

NEW DRUGS; INCRETIN EFFECTS 122
, enhance glucose-dependent insulin")
INCRETIN EFFECT � � Incretins, such as glucagon-like peptide-1 (GLP 1), enhance glucose-dependent insulin secretion and exhibit other antihyperglycemic actions following their release into the circulation from the gut. Incretins 1. 2. 3. enhances glucose-dependent insulin secretion by the pancreatic beta-cell suppresses inappropriately elevated glucagon secretion slows gastric emptying 123

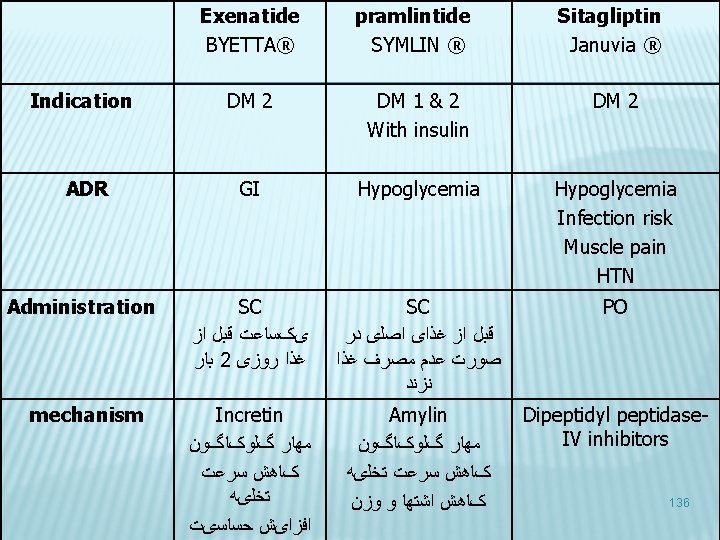
BYETTA™ EXENATIDE 124

BYETTA™ EXENATIDE; MECHANISM � BYETTA improves glycemic control by reducing fasting and postprandial glucose concentrations in patients with type 2 diabetes � Glucose-dependent insulin secretion � BYETTA has acute effects on pancreatic beta-cell responsiveness to glucose and leads to insulin release only in the presence of elevated glucose concentrations. 125

DOSE AND ADR � The most common adverse effects are nausea, vomiting, and diarrhea. � The initial dose is 5 mcg subcutaneously twice daily, titrated to 10 mcg twice daily in 1 month if needed and as tolerated � It should be injected 0 to 60 minutes before the morning and evening meals. 126

BYETTA; PLACE IN THERAPY � Diabetes type 2 � Exenatide should be used as adjunctive therapy in patients who have not achieved adequate glycemic control despite treatment with metformin, a sulfonylurea, and/or a thiazolidinedione. 127

SYMLIN® PRAMLINTIDE 128
 is an antihyperglycemic drug for use in patients with diabetes treated")
SYMLIN® (PRAMLINTIDE ACETATE) is an antihyperglycemic drug for use in patients with diabetes treated with insulin � Pramlintide is a synthetic analog of human amylin, a naturally occurring neuroendocrine hormone synthesized by pancreatic beta cells that contributes to glucose control during the postprandial period. � SYMLIN is formulated as a clear, isotonic, sterile solution for subcutaneous (SC) administration � 129

INDICATIONS AND USAGE Type 1 diabetes, as an adjunct treatment in patients who use mealtime insulin therapy and who have failed to achieve desired glucose control despite optimal insulin therapy. � Type 2 diabetes, as an adjunct treatment in patients who use mealtime insulin therapy and who have failed to achieve desired glucose control despite optimal insulin therapy, with or without a concurrent sulfonylurea agent and/or metformin � 130

MECHANISM AND EFFECT � Pramlintide suppresses 1. 2. 3. § inappropriately high postprandial glucagon secretion reduces food intake (which can cause weight loss) slows gastric emptying Pramlintide decreases prandial glucose excursions but has little effect on FPG concentrations 131

PRAMLINTIDE � The most common adverse effects are nausea, vomiting, and anorexia. � It does not cause hypoglycemia when used alone, but it is indicated only in patients receiving insulin, so hypoglycemia can occur. 132

DIPEPTIDYL PEPTIDASE-IV INHIBITORS Dipeptidyl peptidase-IV inhibitors prolong the halflife of an endogenously produced glucagon-like peptide-1. � These agents partially reduce the inappropriately elevated glucagon postprandially and stimulate glucosedependent insulin secretion. � The average reduction in A 1 C is approximately 0. 7% to 1% at a dose of 100 mg/day. � 133

ADR � The drugs are well tolerated, weight neutral, and do not cause GI side effects. � Mild hypoglycemia appears to be the only significant adverse effect, but long-term safety data are limited. 134
 � Tablet: 25 mg, 50 mg, 100 mg � Sitagliptin (Januvia) is")
SITAGLIPTIN (JANUVIA®) � Tablet: 25 mg, 50 mg, 100 mg � Sitagliptin (Januvia) is usually dosed at 100 mg orally once daily. � In patients with renal impairment, the daily dose should be reduced to 50 mg (creatinine clearance 30– 50 m. L/min) or 25 mg (creatinine clearance <30 m. L/min). 135

137

139

NEUROPATHY In diabetes, a complex array of metabolic, vascular and perhaps hormonal factors shift the balance between nerve fiber damage and nerve fiber repair in favor of the former. � This pattern preferentially affects distal sensory and autonomic fibers, leading to the progressive loss of sensation that underlies the clinical manifestations of diabetic polyneuropathy. � 141

NEUROPATHY � 1. 2. Involvement of the peripheral and autonomic nervous systems is probably the most common complication of diabetes. Autonomic neuropathy Peripheral neuropathy 142

AUTONOMIC NEUROPATHY 143

NEUROPATHY � GENITOURINARY AUTONOMIC NEUROPATHY � Gastroparesis � cardiovascular � Neuropathic pain 144

PERIPHERAL NEUROPATHY � 1. 2. 3. There are three main elements in the treatment regimen: Glycemic control Treatment of pain Foot care 145

GLYCEMIC CONTROL � The most important treatment for the prevention of diabetic neuropathy is optimal glucose control 146

NEUROPATHIC PAIN � TCA � Anticonvulsants � Duloxetine � Capsaicin � Anesthetic drugs 147

148
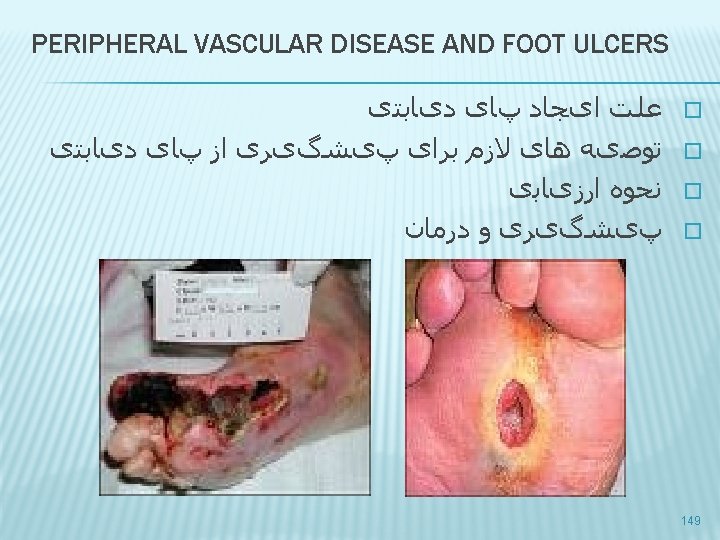

DIABETIC FOOT; CAUSE Both vascular and neurologic disease contribute to this problem � it promotes ulcer formation by � decreasing pain sensation and perception of pressure � impairing the microcirculation and the integrity of the skin � causing muscle imbalance that can lead to anatomic deformities � � Once ulcers form, healing may be delayed or difficult to achieve, particularly if infection penetrates to deep tissues and bone and/or there is diminished local blood flow. 150

PERIPHERAL VASCULAR DISEASE AND FOOT ULCERS Claudication and nonhealing foot ulcers are common in type 2 DM patients. � Smoking cessation, correction of lipid abnormalities, and antiplatelet therapy are important strategies in treating claudicants. � Pentoxifylline or cilostazol can be useful in selected patients. � Revascularization is successful in selected patients. � Local débridement and appropriate footwear and foot care vitally important in the early treatment of foot lesions. 151 �

ﺍﺭﺯیﺎﺑی � Neuropathy � Vibration sensation � Pressure sensation � Superficial pain or temperature sensation � peripheral arterial disease � cool temperature � the absence of hair � lower limb pulses 152

GENERAL TREATMENT � Extensive debridement � good local wound care � relief of pressure on the ulcer � Close monitoring is required, and hospitalization for bed rest and intravenous antibiotic therapy is advisable if the ulcer does not improve. 155

CILOSTAZOL � phosphodiesterase inhibitor approved by the FDA for the treatment of intermittent claudication. � It suppresses platelet aggregation and is a direct arterial vasodilator � treatment with 100 mg twice daily for 12 to 24 weeks increased maximal and pain-free walking distances by 50 and 67 percent respectively 156

CILOSTAZOL � Cilostazol appears to be more effective than pentoxifylline. Side effects included headache, loose and soft stools, diarrhea, dizziness and palpitations. � Because other oral phosphodiesterase inhibitors used for inotropic therapy have caused increased mortality in patients with advanced heart failure, cilostazol is contraindicated in heart failure of any severity � 157

CILOSTAZOL � Cilostazol should be taken one-half hour before or two hours after eating, because high fat meals markedly increase absorption � Several drugs such as diltiazem and omeprazole, as well as grapefruit juice, can increase serum concentrations of cilostazol if taken concurrently 158
 � Pentoxifylline is a rheologic modifier approved by the Food and")
PENTOXIFYLLINE (TRENTAL) � Pentoxifylline is a rheologic modifier approved by the Food and Drug Administration (FDA) for the symptomatic relief of claudication � Its putative mechanism of action includes an increase in red blood cell deformity, and decreases in fibrinogen concentration, platelet adhesiveness, and whole-blood viscosity. 159

NEPHROPATHY � To reduce the risk or slow the progression of nephropathy, optimize glucose control. � To reduce the risk or slow the progression of nephropathy, optimize blood pressure control. 160
 in type 1")
SCREENING Perform an annual test to assess urine albumin excretion (UAE) in type 1 diabetic patients with diabetes duration of 5 years and in all type 2 diabetic patients, starting at diagnosis. � Measure serum creatinine at least annually in all adults with diabetes regardless of the degree of UAE. � The serum creatinine should be used to estimate GFR and stage the level of chronic kidney disease (CKD), if present. � 161

TREATMENT ; ACEI & ARB In patients with type 1 diabetes, with hypertension and any degree of albuminuria, ACEI have been shown to delay the progression of nephropathy � In patients with type 2 diabetes, hypertension, and microalbuminuria, both ACEI and ARBs have been shown to delay the progression to macroalbuminuria. � In patients with type 2 diabetes, hypertension, macroalbuminuria, and renal insufficiency (serum creatinine 1. 5 mg/dl), ARBs have been shown to delay the progression of nephropathy. � If one class is not tolerated, the other should be 162 substituted. �

RETINOPATHY SCREENING AND TREATMENT � To reduce the risk or slow the progression of retinopathy, optimize glycemic control. � To reduce the risk or slow the progression of retinopathy, optimize blood pressure control. 163

SCREENING � � Adults and children aged 10 years or older with type 1 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist within 5 years after the onset of diabetes. Patients with type 2 diabetes should have an initial dilated and comprehensive eye examination by an ophthalmologist or optometrist shortly after the diagnosis of diabetes. Subsequent examinations for type 1 and type 2 diabetic patients should be repeated annually by an ophthalmologist or optometrist. Less frequent exams (every 2– 3 years) may be considered following one or more normal eye exams. 164

TREATMENT � refer patients with any level of macular edema and other disorder to an ophthalmologist � Laser photocoagulation therapy is indicated to reduce the risk of vision loss in patients with high-risk and clinically significant macular edema. � The presence of retinopathy is not a contraindication to aspirin therapy for cardioprotection, as this therapy does not increase the risk of retinal hemorrhage 165

RETINOPATHY & NEPHROPATHY Control of BS and BP!! 166

HYPERTENSION/BLOOD PRESSURE CONTROL � Screening and diagnosis � Blood pressure should be measured at every routine diabetes visit. � Patients found to have SBP 130 mm. Hg or DBP 80 mm. Hg should have blood pressure confirmed on a separate day. � Repeat SBP 130 mm. Hg or DBP 80 mm. Hg confirms a diagnosis of hypertension. 167

GOALS � Patients with diabetes should be treated to a systolic blood pressure <130 mm. Hg. � Patients with diabetes should be treated to a diastolic blood pressure <80 mm. Hg. 168

DRUG THERAPY DRUGS OF CHOICE Pharmacologic therapy should be with a regimen that includes either an ACEI or an ARB. � If one class is not tolerated, the other should be substituted. � If needed to achieve blood pressure targets, a thiazide diuretic should be added to those with an estimated glomerular filtration rate (GFR) >30 ml/min per 1. 73 m 2 and a loop diuretic for those with an estimated GFR 30 ml/min per 1. 73 m 2 � 169

DYSLIPIDEMIA/LIPID MANAGEMENT � Screening: � In most adult patients, measure fasting lipid profile at least annually. � In adults with low-risk lipid values lipid assessments may be repeated every 2 years. 170

STATIN THERAPY � Statin therapy should be added to lifestyle therapy, regardless of baseline lipid levels, for diabetic patients: 1. 2. 3. with overt CVD without CVD who are over the age of 40 years and have one or more other CVD risk factors. Expect above if LDL cholesterol remains above 100 mg/dl or in those with multiple CVD risk factors 171

172

ANTIPLATELET AGENTS � Indication 1. 2. High risk patients Secondary prevention 173

ANTIPLATELET AGENTS; ASPIRIN IN HIGH RISK PATIENTS � � Consider aspirin therapy (75– 162 mg/day) as a primary prevention strategy in those with type 1 or type 2 diabetes at increased cardiovascular risk (10 year risk >10%). This includes most men>50 years of age or women>60 years of age who have at least one additional major risk factor � � � Family history of CVD Hypertension Smoking Dyslipidemia albuminuria 174
 as")
SECONDARY PREVENTION; ASPIRIN IN SECONDARY PREVENTION � Use aspirin therapy (75– 162 mg/day) as a secondary prevention strategy in those with diabetes with a history of CVD. 175

CLOPIDOGREL AND COMBINATION THERAPY � For patients with CVD and documented aspirin allergy, clopidogrel (75 mg/day) should be used. � Combination therapy with ASA (75– 162 mg/day) and clopidogrel (75 mg/ day) is reasonable for up to a year after an acute coronary syndrome. 176
 PATIENTS WITH KNOWN CVD � � In patients with known")
CORONARY HEART DISEASE (CHD) PATIENTS WITH KNOWN CVD � � In patients with known CVD this drugs should be used (if not contraindicated) to reduce the risk of cardiovascular events: 1. ACE inhibitor 2. Aspirin 3. Statin therapy (A) In patients with a prior myocardial infarction, add beta-blockers (if not contraindicated) to reduce mortality. 177
- Slides: 178