1 Cardiac Pacemakers Implantable Cardioverter Defibrillators ICD Dr

1
 Dr Majid Shojaee Associate professor of EM")
Cardiac Pacemakers & Implantable Cardioverter Defibrillators (ICD) Dr Majid Shojaee Associate professor of EM EHMC SBMU 2

The Pacemaker System Patient Lead n Pacemaker • Programmer n Lead Pacemaker 3

4

Pacemaker Nomenclature 1 st letter – chamber paced 2 nd letter – chamber sensed 3 rd letter – Response to chamber sensed 5

Pacemaker Nomenclature I II IV V Chamber Paced Chamber Sensed Response to Sensing Rate Modulation, Programmability Antitachycardia Features A=Atrium T=Triggered P=Simple P=Pacing V=Ventricle V=Ventricl e I=Inhibited M=Multiprogrammable S=Shock D=Dual (A & V inhibit. ) R=Rate Adaptive D=Dual (shock+ pace) O=None C=Communicating O=None 6

7

LAD +BBB =LBBB Sinus node AV node Like a Conduction block Stimulation 8
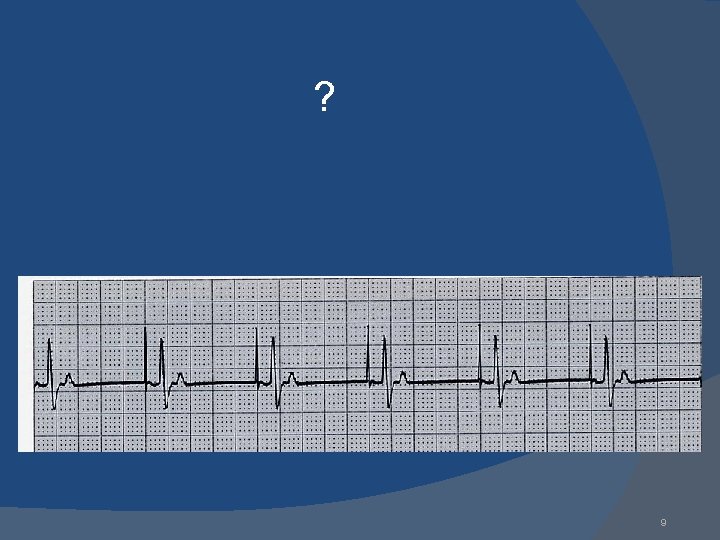

Normal Pacing Atrial Pacing Atrial pacing spikes followed by P waves 10

? 11

Normal VVI 12

? 13

DDD 14

channel marker 15

? 16

Normal DDD A-V Pacing Atrial & Ventricular pacing spikes followed by atrial & ventricular complexes 17

18

19

20

21

Complication of implantation Infection Thrombophlebitis Pacemaker syndrome Pacemaker malfunction: Ø Failure to output Ø Ø Failure to capture Undersensing Oversensing Inappropriate pacemaker rate 22

23

? 24

non-capture Atrial non-capture Atrial pacing spikes are not followed by P waves 25

FAILURE TO CAPTURE in VVI 26

? 27

non-capture Ventricular non-capture Ventricular pacing spikes are not followed by QRS complexes 28

? 29

undersensing Ventricular undersensing Ventricular pacing spikes occur regardless of QRS complexes Pacemaker is not “seeing” intrinsic activity 30
 31")
Failure to sense (undersensing) 31

? 32

Undersensing AAI An intrinsic depolarization that is present, yet not seen or sensed by the pacemaker P-wave not sensed Atrial Undersensing (OVERPACING) 33

? 34
 for paced ventricular")
Failure to Sense & Failure to Capture Danger – potential (low) for paced ventricular beat to land on T wave 35

36

Oversensing The sensing of an inappropriate signal Can be physiologic or nonphysiologic If a pacemaker is oversensing, you will see signals on the marker channel that do not correspond to the ECG pattern 37

Pacemaker Complications Pacemaker syndrome Patient feels worse after pacemaker placement Presents with progressive worsening of CHF symptoms Due to loss of atrioventricular synchrony, pathway now reversed and ventricular origin of beat 38

“Pacemaker Syndrome” Fatigue, dizziness, hypotension Caused by pacing the ventricle asynchronously, resulting in AV dissociation or VA conduction Mechanism: atrial contraction against a closed AV valve and release of atrial natriuretic peptide Worsened by increasing the ventricular pacing rate, relieved by lowering the pacing rate or upgrading to dual chamber system Therapy with fludrocortisone/volume expansion NOT helpful 39
 can")
ACLS Interventions Electrical defibrillation at recommended shock strengths (200, 300, and 360 J) can be safely performed in the patient with a pacemaker. it is a safe distance(>10 cm) from the pulse generator. alternatively, defibrillation electrodes can be placed in an antroposterior configuration A chest radiograph should also be obtained after resuscitation to ensure that the pacing catheter was not displaced during chest compression. Immediate return of pacing(capture)may not occure after defibrillation; (global myocardial ischemia_malfunction of pacemaker) therefor temporary transcutaneous pacing may be needed 40

41

Magnet Inhibition Closes an internal reed switch Causes sensing to be inhibited Temporarily turns pacemaker into “asynchronous” mode (set rate) Does NOT turn pacemaker off Rate can confer info regarding battery life 42

Magnet 43

Practice Strip#1 44

Practice Strip #2 45

Practice Strip #3 46

Practice Strip #4 47

Practice Strip #5 48

Practice Strip #6 49

Practice Strip #7 DDD 50

Practice Strip #8 51

Practice Strip #9 52

Answers 1. 2. 3. 4. 5. 6. 7. 8. 9. AAI: normal atrial pacing Sinus rhythm: no pacing; possible inhibitory backup DDD: failure to sense ventricle; VVI: ventricular pacing DDD: failure to capture atria or ventricle; DDD: normal atrial & ventricular pacing DDD: normal atrial sensing, ventricular pacing DDD: failure to capture atria; DDD: oversensing; 53

AICD 54

Implantable Cardioverter Defibrillators 55

Many patients still require drug therapy after ICD implantation to Suppress ventricular dysrhythmias, Minimize the frequency of ICD shocks, Improve patients’ tolerance, and Decrease energy use, which prolongs ICD life. 56

VT Optimally, the required shock strength for defibrillation is less than half the maximum output (approximately 30 J) of the device. VT is typically managed with use of either low-energy shocks or antitachycardia pacing that interrupts the VT reentrant circuit. 57

VF In the setting of VF, ICDs are capable of delivering up to five additional shocks if the first shock fails. 58

Hedges Antiarrhythmic medications may be required for a resistant malignant rhythm when the AICD is functioning properly but the arrhythmia persists 59
")
Malfunction The most common complaint of ICD patients is occurrence of frequent shocks (Oversensing) 60

Oversensing An increase in the shock frequency is a manifestation of ICD sensing malfunction if (1) a supraventricular tachyarrhythmia is inappropriately sensed as VT, (2) shocks are delivered for nonsustained VT (3) intracardiac T waves detected by the ICD system are sensed as QRS complexes and the ICD interprets this as an increased heart rate. 61

Temporary ICD deactivation with magnet application may be necessary if oversensing is the problem 62

Undersensing Syncope, near-syncope, dizziness, or lightheadedness in the patient with an ICD may indicate undersensing of sustained VT or inappropriately low shock strength to terminate the rhythm. 63

Complications of implantation Infection of the wound and subcutaneous pouch fashioned for the divice Thrombophlebitis Chronic thrombosis of the veins traversed for lead insertion 64

Temporary ICD deactivation with magnet application may be necessary if oversensing is the problem. Syncope, near syncope, dizziness , or lightheadedness in the patient with an ICD may indicate undersensing of sustained VT or inappropriately low shock strength to terminate the rhythm. 65

ACLS Interventions An ICD does not prevent sudden death in all patients at risk, Transthoracic defibrillation can be performed (200, 360 J) (location about 10 cm from ICD subcutaneous pouch). If the ICD discharges during manual chest compressions, the rescuer may feel a weak shock. (no report of injury to rescuer. (harmless) The divice can be deactivated with magnet. (corner) Post resuscitation rhythms treated with (lidocaine, amiodarone) 66

External cardiac defibrillation may be performed safely Pads be placed at a location approximately 10 cm distant. If available, biphasic cardioverter-defibrillators If successful resuscitation: the pacemaker or AICD should be interrogated expeditiously by a cardiologist or electrophysiologist 67

Bi-Ventricular Pacing Right atrial lead Coronary sinus lead Right ventricular lead N Engl J Med 2003 68

Bi-V Pace 69

70

CARDIAC ASSIST DEVICES Mechanical ventricular assistance devices have been used as a “bridge” to transplantation since the 1960 s. Newer devices, such as the Jarvik 2000 and Heart. Mate II, are continuous flow pumps… 71

The LVAD supports the patients cardiac output via a mechanical pump that draws blood from an inflow cannula in the left ventricle and pumps it into the ascending aorta via an outflow cannula. 72

Significantly with 2 year survival in over half of pts. The greatest mortality is noted within the first 30 days after implantation and during hospitalization. 73
, Biventricular assist device (Bi. VAD) and Total")
Three types: Left ventricular assist device (LVAD), Biventricular assist device (Bi. VAD) and Total artificial heart (TAH). 74

Patients with LVADs require lifelong anticoagulation to prevent the graft from clotting. Most patients also have a pacemaker or automatic implanted cardiac defibrillator (AICD) placed. 75

The most common LVADs produce a non-pulsative flow, Therefore patients are essentially pulseless making traditional hemodynamic vital sign interpretation impossible 76

Blood pressure may be measured using a manual cuff with a Doppler probe over the radial or brachial artery. The cuff pressure is reduced until a constant sound is heard. The pressure at this point represents the mean arterial pressure. Blood pressure can also be measured invasively using an arterial catheter. 77

Chest compressions risk dislodging the device, resulting in massive hemorrhage, Although a recent case series of eight patients with LVAD who received chest compressions showed no cannula dislodgements with four patients surviving the initial arrest. 78

Prior to considering chest compressions, multiple methods should be used to confirm absence of circulation, and attempts should be made to correct mechanical pump malfunction. In some devices, the hand pump can be used to provide backup circulation, and early transition to cardiopulmonary bypass should be considered 79
 produces pulsatile flow. Because the native heart")
The currently available TAH (Syn. Cardia) produces pulsatile flow. Because the native heart has been removed, 80
; therefore defibrillation and pacing")
patients with a TAH have no cardiac electrical activity (asystole); therefore defibrillation and pacing are never indicated. Chest compressions are not effective with the TAH and could be harmful due to traumatic disruption of the heart or drive lines. 81

Epinephrine and vasopressin are generally not recommended for TAH patients, because there is no native heart to respond. 82
- Slides: 82